 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 - May 2019
Sadananjali1*, Manasa D R2
1Assistant Professor, Department of Biochemistry, KBN Institute of Medical Sciences, Kalaburgi, Karnataka, INDIA. 2Tutor, Department of Biochemistry, Belagavi Institute of Medical Sciences, Belagavi, Karnataka, INDIA. Email: hukkeri.anjali@gmail.com
Abstract Background: Recent data have suggested that serum uric acid (SUA) level is positively associated with the development of type 2 diabetes (T2DM). We also know that diabetes is also independent risk factor for cardiovascular diseases. Objectives: To study the relationship between glycemic control and serum uric acid level in Acute MI cases. Material and Methods: A prospective cross sectional study on 100 AMI cases done at tertiary care intensive unit. They were divided into two groups, group I with only AMI cases and group II with AMI cases having poor glycemic control. Data was analyzed using SPSS and mean, SD and p value was calculated. Results: Out of 100 cases 62% cases were males and 38% cases were female in this study. Mean age of study was 53.7 ± 15.7 years. The mean serum uric acid level in group I was 5.26 mg/dl and in group II was 5.17 mg/dl. There was no any significant association (p >0.05) between serum uric acid levels in both the groups. The mean blood glucose level in group I was 113.4 mg/dl and in group II it was 283.7 mg/dl. The glucose level was significantly higher (p ˂0.05) in group II when compared with group I. The mean HbA1c level in group I was 5.12% while in group II it was 8.79%. There was significantly higher (p ˂0.05) HbA1c seen in group II. Conclusions: More research in this regards should be done. Key Word: Serum Uric Acid, Hyperglycemia, Myocardial Infarction
INTRODUCTION Acute myocardial infarction (AMI) has already established itself as a major risk to health both in developed and developing nations.1,2Recent studies concludes that concentrations of serum uric acid can be a cheap and easy-to-obtain indicator of cardiovascular risk.3,4Serum uric acid levels are increased in patients with ischemic heart disease. Levels also increase with age, obesity, high alcohol consumption, combined hyperlipidemias, diabetes mellitus and hypertension. These cluster of abnormalities in turn significantly increase the risk of atherosclerotic vascular diseases like myocardial infarction (MI) and stroke.5 Diabetes mellitus (DM) can be described as a group of disorders of carbohydrate metabolism in which glucose is produced in large amounts, leading to hyperglycemia.6Diabetes increases the risk of cardiovascular disease and stroke, about 50% of people with diabetes die of cardiovascular disease.7 Hyperglycemia acts as a multiplier of cardiovascular risk and is implicated in vascular damage and cardiac myocyte death through different molecular mechanisms.8Little is known on the association between uric acid and stroke risk: an association was found between uric acid and stroke risk in diabetics9 and between uric acid and fatal stroke in the general population.10 Also there are less studies on this topic so we conducted this to study the relationship between glycemic control and serum uric acid level in Acute MI cases.
MATERIAL AND METHODS This was a prospective cross sectional study conducted on AMI cases at ESIC Medical College, Kalaburgi, Karnataka, who were admitted in intensive care unit of this hospital. This study was conducted for a period of 1 year. Inclusion criteria: All the cases presenting with AMI at intensive care unit, aged above 20 years, AMI with diabetes taken as control group, those who have given consent for this study. Exclusion criteria: All those without AMI, with known systemic disorder other than cardiovascular and diabetes, all those who did not give consent. Cases were divided into two groups namely group I (50) with AMI alone and group II (50) those with AMI and poor glycemic control (≥8% HbA1c). The diabetic patients were classified as per HbA1c level.11Informed consent was taken from patients or from their families. Detailed history was taken with the help of preformed proforma. For sample collection, venous blood taken after overnight fasting, serum separated. Simultaneously, blood samples were collected in ethylenediaminetetraacetic acid anticoagulation tubes for HbA1c estimation. HbA1c was estimated by Turbidimetric inhibition immunoassay method12 and Serum Uric acid by Uricase Method.13 study was approved by the ethics committee. Data was analyzed using SPSS version 20 and percentage mean, SD, p value was calculated. p ˂0.05 taken as significant finding. RESULTS Diagram 1: Gender wise distribution of cases 62% cases were males and 38% cases were female in this study. Mean age of study was 53.7±15.7 years.
Table 1: Distribution of cases as per parameters
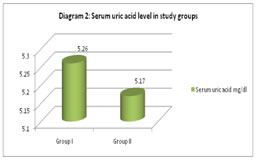
The mean value of serum uric acid in group I was found to be 5.26 (1.32-9.43)mg/dl, in group II it was 5.17(1.78-10.23)mg/dl. In group I the mean blood glucose level was 113.4 (80-147) mg/dl and in group II it was 283.7 (93-461) mg/dl, in group I the means value of HbA1c % was 5.12 (4.3-6.2)mg/dl and in group II it was found to be 8.79(7.3-11.8)mg/dl. Diagram 2: Serum uric acid level in study groups The mean serum uric acid level in group I was 5.26 mg/dl and in group II was 5.17 mg/dl. There was no any significant association (p >0.05) between serum uric acid levels in both the groups.
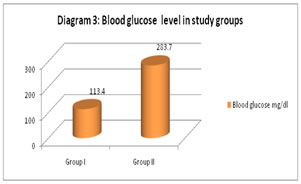
Diagram 3: Blood glucose level in study groups The mean blood glucose level in group I was 113.4 mg/dl and in group II it was 283.7 mg/dl. The glucose level was significantly higher (p ˂0.05) in group II when compared with group I.
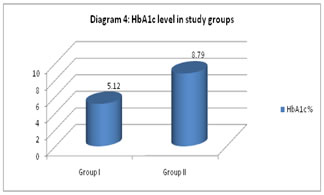
Diagram 4: HbA1c level in study groups The mean HbA1c level in group I was 5.12% while in group II it was 8.79%. There was significantly higher (p ˂0.05) HbA1c seen in group II.
DISCUSSION This a prospective cross sectional study done on 100 cases with AMI. In this study out of total 100 cases 62% cases were males and 38% cases were female. Mean age of study was 53.7 ± 15.7 years. This result was in accordance with Burki L et al14 in their study males formed 70% and females formed 30% of the study. The mean age of Burki L et al14 study was found to be 50.0±12.4, this was similar with our study. While higher mean age of 61 yearsand 62.6 was seen with Forman JPet al15 and Hajizadeh R et al.16 In our study we did not find any significance between serum uric acid and glycemic control in infarction cases. Cirakli ZL et al17and Biswas K et al18also concluded the same. However, unlike our study Quiñones Galvan A et al19 found significant association between uric acid and glycemic control in AMI cases. There was no any statistically significant association between the HbA1c level and the uric acid level in any of our study groups. Higher glucose was seen in AMI cases in Lv et al20In this study, we can say that the serum uric acid level on raise with increase in fasting plasma glucose in group I, but seems to be decreasing in group II. This was found to be similar with Cirakli ZL et al17 and Nan H et al21studies. According to few studies it is said that hyperuricemia increases the risk of developing diabetes in patients with hypertension.21It is still not clear about role of uric acid and cardiovascular risk. Sluijset al.22 concluded that uric acid-lowering drugs may not be helpful in decreasing the risk of developing diabetes.
CONCLUSION This study was a observational cross sectional study, so we cant generalize findings. A randomized control trial would have been better with larger sample size. There was significant association between blood glucose and HbA1c and AMI in two groups, but there was no significant association between serum uric acid and AMI in two groups in our study, further research is advisable.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.