 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 3 - June 2019
Transfusion associated hemoglobinopathy
Minal Pore1*, Pramod Ingale2, Dipti Tiwari3, Shubhangi Wankhade4
1,4 Sr. Resident, 2Professor & HOD, Department of Biochemistry, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, INDIA. 3Assistant Professor, Department of Biochemistry, Grant Medical College and Sir J.J. Group of Hospitals, Mumbai, INDIA. Email: minalpore33@gmail.com
Abstract Transfusion associated hemoglobinopathy occurs when the donor is an asymptomatic carrier of the abnormal haemoglobin and such blood is transfused to a patient. Abnormal peaks are seen in High Performance Liquid Chromatography causing diagnostic dilemmas. Here we report one such case of transfusion associated hemoglobinopathy. Key Word: High performance liquid chromatography (HPLC), Hb S hemoglobinopathy, transfusion peaks.
INTRODUCTION Transfusion associated hemoglobinopathy is of concern as it leads to misdiagnosis, repeated testing, delay in treatment and may lead to adverse consequences to the patient.1 It occurs when the donor is an asymptomatic carrier of the abnormal haemoglobin and such blood is transfused to a patient.2,11 Abnormal peaks appear in HPLC leading to diagnostic dilemmas.2,4 Here is a case of HbS hemoglobinopathy due to transfusion.
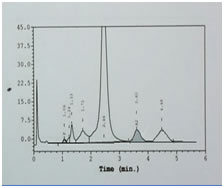
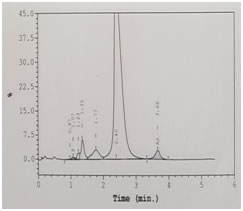
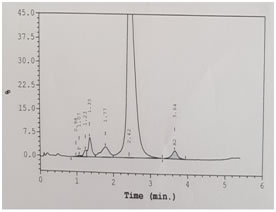
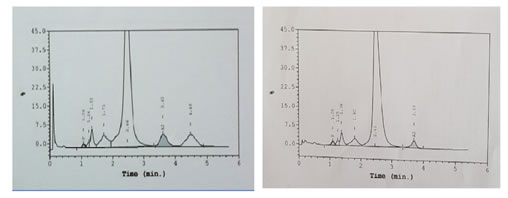
CASE REPORT A 3-year-old male child was brought to paediatric O.P.D. with the complaints of recurrent fever, joint pains and lethargy since 15 days. On examination the child was conscious, oriented, had average built, pallor +++, tachycardia present, no petechiae or active bleeding was present. The haematological investigations like Hb, CBC and Hb variant testing to rule out possibility of hemoglobinopathy were advised. Hb was 6gm/dl and peripheral smear showed microcytic hypochromic red cell picture [Table 1]. Hb HPLC (BioRad Variant II, βthalassemia Short Program) showed a HbF level of 1.1%, HbA2 3.5% and a peak in S window of 4.9% [Figure 1]. Both parents chromatograms were normal. [Figure 2 and 3] & there was no abnormal peak of S window in both the parents. This lead to further diagnostic confusion. Detailed discussion was done with the referring clinician and lab obtained detailed patient history. There was a history of blood transfusion to the patient 2 weeks prior to sending the sample for Hb-HPLC. We thought this could be the major reason for altered variants in this patient. The clinician was informed to repeat the test after 4 weeks. After 4 weeks the chromatogram was normal, & did not show any S window. Table 1: CBC Findings
Table 2: PBS Picture
Table 3:
Table 4:
Table 5:
Figure 1: Patient's chromatogram Figure 2: Parents' chromatogram Figure 3: Chromatogram of patient before and after DISCUSSION Sickle cell trait is a condition in which the patient has one abnormal haemoglobin beta gene allele (heterozygous), but doesn't have symptoms like that of sickle-cell disease patient (homozygous). Prevalence of sickle cell trait is as high as 13% in certain Indian communities.5 As the blood bank criteria for donor selection do not include any screening tests for detection of such carriers and they are asymptomatic, it is likely that blood from a Sickle cell trait donor can be transfused to any patient. In our study, the Hb variant status of the donor lead to changes in Hb-HPLC report of the recipient which caused confusion, misdiagnosis and delay in proper treatment. The case was subsequently resolved by the low percentage of abnormal Hb, transient nature of peaks and normal chromatograms of other family members. Somasundaram et al. in the year 2015 have reported an incidence of transfusion acquired HbS hemoglobinopathies of 8.5% in a 16 year old male, causing diagnostic dilemma.6 Kozarski et al. in the year 2006, have reported apparent hemoglobinopathies with transfusion associated peaks in 32 recipients, HbC being the most common transfused Hb detected in their study. The % of abnormal Hb was in the range of 0.8-14%. 7 Gupta et al. in the year 2011 showed in their study, three cases of Hb variant HPLC out of 1530 cases had apparent post-transfusion hemoglobinopathy with HbS % in the range of 9.9–18.5%. 8 Rarely, transfusion of abnormal HbS can lead to life threatening complications as shown in the study by Nowak et al. In their study, a neonate was transfused with blood from a sickle cell trait donor, which resulted in multiple renal and splenic infarcts in the baby.9 It is important to make the diagnosis of a hemoglobinopathy but it is also important to avoid misdiagnosis. This was shown in the study by Wong et al. (2010). In their case a normal individual was misdiagnosed as heterozygous β-thalassemia after receiving transfusion from HbE carrier.10
CONCLUSION It is concluded that careful history of blood transfusion should be obtained before sending and processing of samples for Hb variants testing. It is recommended that there should be a gap of around three months between the last blood transfusion and Hb variants testing by HPLC to avoid erroneous results.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.