 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 1 - July 2019
Dyslipidaemia in patients with central obesity having metabolic syndrome
Saba Nazneen Khan1*, Mirza Sharif Ahmed Baig2, Mohd Abdul Baseer3, Anant A Takalkar4
1Assistant Professor, 2Professor and HOD, Department of Biochemistry, Khaja Banda Nawaz Inst. Of Medical Sciences, Kalaburagi, INDIA. 3Associate Professor, Department of Community Medicine, Khaja Banda Nawaz Inst. Of Medical Sciences, Kalaburagi, INDIA. 4Professor, Department of Community Medicine, MIMSR Medical College, Latur, Maharashtra, INDIA. Email: naazdr@ymail.com
Abstract Background: Blood cholesterol has long been recognized as a major independent risk factor for CVD in adults. More recently, the level of triglycerides (TG) has been incriminated as a CVD risk factor independent of cholesterol. Objective: To study lipid profile in patients with central obesity with metabolic syndrome and to compare with controls. Methodology: Case control study was conducted at Navodaya Medical College Hospital and Research Centre, Raichur from April 2013 to May 2014. Patients attending outpatient Department and those admitted were included in the study. The patients and controls had voluntarily participated in the study. Present study comprised of 100 patients which includes 50 cases of metabolic syndrome and 50 controls. Results: 48.27% of males and 47.62% of females of range 45 – 50years of age were taken in the study as cases. The mean ± SD of serum TG in cases and controls were 191.20 ±87.63 and 108.01± 25.95 respectively. The mean ± SD of serum HDL- Cholesterol in cases and controls were 38.74 ± 9.46 and 57.2± 12.30 respectively. The mean ± SD of serum LDL- Cholesterol in cases and controls were 132.79 ± 59.35 and 90.65 ± 30.52 respectively. The mean ± SD of serum VLDL-Cholesterol in cases and controls were 38.07 ± 17.50 and 23.12± 12.78 respectively. Conclusion: we observed that serum total cholesterol, triglycerides, LDL and VLDL are significantly higher in cases i.e. obese with metabolic syndrome as compared to controls. Key words: Metabolic syndrome, dyslipidemia.
INTRODUCTION In India, CVD accounts for 31.7% of total deaths. In developing countries, mortality due to CVD is expected to rise to 19 million by 2020. In the Indian subcontinent, CVD manifests itself almost 10 years earlier on an average compared with the rest of the world, in western countries, CVD accounts for only 23% of the CVD deaths occurring below the age of 70 compared to 52% of CVD deaths below the age of 70 in India.1 The association between dyslipidemia, obesity, and hypertension is well established and all have been found to be major risk factors for the development of CVD, a leading cause of visits to physicians and cause of death. 2,3,4Blood cholesterol has long been recognized as a major independent risk factor for CVD in adults. More recently, the level of triglycerides (TG) has been incriminated as a CVD risk factor independent of cholesterol.5Obesity is considered a chronic (long-term) disease, like high blood pressure or diabetes. It has many serious long-term consequences for health, and it is the second leading cause of preventable deaths in many countries. Although the exact biochemical mechanisms responsible for the association between obesity and the above diseases have not been completely elucidated, it is known that increase in triglyceride stores is associated with a linear increase in the production of cholesterol which in turn is associated with increased cholesterol secretion in bile and an increased risk of gallstone formation and the development of gall bladder diseases. 6, 7
OBJECTIVE To study lipid profile in patients with central obesity with metabolic syndrome and to compare with controls.
METHODOLOGY A case control study was conducted at Navodaya Medical College Hospital and Research Centre, Raichur from April 2013 to May 2014. Patients attending outpatient Department and those admitted were included in the study. The patients and controls had voluntarily participated in the study. Present study comprised of 100 patients which includes:-50 cases with Metabolic Syndrome [Clinically diagnosed/confirmed cases of HTN and/ or DM/ glucose intolerance with central obesity (waist circumference ≥ 90cm (males), ≥ 80cm (female)].50 were healthy controls. The patients were between the age group of 20– 50 years. Inclusion criteria:
Exclusion criteria:
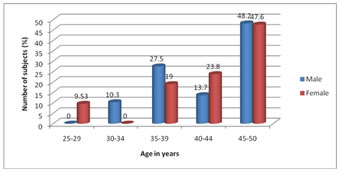
The duration of the study was from April 2013 to may 2014. Statistical analysis was carried out using student ‘t’ test (unpaired). RESULTS Figure 1: Age and Sexwise wise distribution of cases 9.53% of females ranging between 25- 29 years, 10.35 % of males and 0% of females ranging between 30 – 34 years, 27.58% of males and 19.05% of females of ranging between 35- 39years, 13.79% of males and 23.8% of females ranging between 40 – 44years, 48.27% of males and 47.62% of females of range 45 – 50years of age were taken in the study as cases. Table 1: Comparison of lipid profile between Cases and Controls (Unpaired “t” test)
The mean ± SD of serum total cholesterol in cases and controls were 209.36 ± 56.55 and 169± 30.84 respectively. The mean ± SD of serum TG in cases and controls were 191.20 ±87.63 and 108.01± 25.95 respectively. The mean ± SD of serum HDL- Cholesterol in cases and controls were 38.74 ± 9.46 and 57.2± 12.30 respectively. The mean ± SD of serum LDL- Cholesterol in cases and controls were 132.79±59.35 and 90.65 ± 30.52 respectively. The mean ± SD of serum VLDL-Cholesterol in cases and controls were 38.07±17.50 and 23.12± 12.78 respectively. Statistically there was highly significant increase (p <0.001) in serum total cholesterol, serum TG, serum LDL- Cholesterol, serum VLDL- Cholesterol and highly significant decrease in serum HDL- Cholesterol of cases as compared to controls. DISCUSSION Table 2: Mean age in various studies
The mean age of males in our study is 42.86±6.31 and females are 52.12±14.99 years and this is comparable with other studies. Age is an important factor as more than 45years of age are at greater the risk of MS. Our findings of age adjusted prevalence are similar to studies conducted by Ramachandran et al.9 and G. P. Parale et al.8 where increasing age had a linear association with MS and its risk factors. Our study showed the there was statistically significant increase in waist circumference of cases as compared to healthy controls. Waist circumference is a good index in assessing of central obesity and also a good predictor tool of insulin resistance. In 2003, Ramachandran et al.9 conducted a study among urban Asian Indian adults to determine the prevalence of metabolic syndrome and in 2005 Dong Feg Gu et al.10 conducted a study to know the prevalence of metabolic syndrome among overweight adults in China. These studies show similar values of waist circumference as compared to our study.
Table 3: Lipid profile in various studies
The characteristic dyslipidemia in metabolic syndrome is elevation of serum TG and decrease in HDL-Cholesterol levels. However, in present study at least one lipid abnormality is present in >95% of cases. HDL-Cholesterol is anti atherogenic (enhances reversed cholesterol transport, anti inflammatory property and ability to protect LDL modification). Obesity itself reduces HDL-Cholesterol levels and the obese patients with metabolic syndrome and atherogenic dyslipidaemia almost always have reduced HDL- Cholesterol. In the year 1996, Mier J et al.12 conducted a study to test whether a predominance of LDL- C and triglycerides levels are independent risk factors for MI. Their findings indicated that nonfasting triglyceride levels appear to be a strong independent predictor of future risk of MI, particularly when total cholesterol level is also elevated. In the year 2011, Ryuichi Kawamoto et al.13 conducted a study to demonstrate association between lipid profiles and metabolic syndrome variables, showing that TG was significantly strongly associated with all three MetS-associated variables in both men and women and concluded that lipid ratios of TG/HDL-C, T-C/HDL-C, LDL-C/HDL-C as well as TG and HDL-C were consistently associated with MetS, insulin resistance and serum HMW Adiponectin. Lipid ratios may be used as reliable markers.
CONCLUSION In our study, we observed that serum total cholesterol, triglycerides, LDL and VLDL are significantly higher in cases i.e. obese with metabolic syndrome as compared to controls. Dyslipidaemia associated with hyperglycemia is a definite risk factor for development of both microvascular and macrovascular complications.
REFERENCES
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.