 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 1 - October 2019
A comparative study of effect of alcohol on Serum Ferritin, LFT and GGT in a tertiary care hospital
B V Mamatha1, Samalad S Vijay Mahantesh2*, D S ShankarPrasad3, S V Kashinakunti4, R Manjula5
1Associate Professor, Department of Biochemistry, Subbaiah Institute of Medical Sciences, Shimoga, Karnataka, INDIA. 2Consultant Paediatric surgeon and Paediatric Urologist, Nanjappa hospital, Kuvempu Road, Shimoga, INDIA. 3,4Professor, Department of Biochemistry, S.N. Medical College, Bagalkot, Karnataka, INDIA. 5Associate Professor, Department of Community Medicine, Bagalkot, Karnataka, INDIA. Email: drmamtha.vijay@gmail.com
Abstract Background: Alcoholism is a serious health issue in majority of developing countries. Oxidative stress due to alcoholism leads to liver injury. Ferritin is an acute phase reactant. The levels of ferritin are found to be elevated in alcoholism. GGT is a marker of alcoholic liver disorders. Objective: To analyse and compare the levels of serum ferritin, LFT markers and GGT in alcoholics and non-alcoholics. Materials and Methods: The study group included 50 patients of alcoholic liver disease and 50 healthy controls who are age and sex matched with cases. Serum ferritin, LFT markers like serum bilirubin, total protein, albumin, AST, ALT, ALP and GGT were estimated in both cases and controls. Results: The study showed that alcoholic patients have significantly increased levels of ferritin, GGT, serum bilirubin, AST, ALT, ALP compared to controls. Serum proteins and albumin levels were significantly lower in cases compared to controls. Serum ferritin showed positive pearson correlation with AST, ALT and GGT. Conclusion: The increased serum levels of ferritin in cases show that oxidative stress in alcoholics is the main cause of liver injury and associated complications with it. Frequent follow up should be done along with the treatment of the disease. It is necessary to give antioxidant supplements to prevent the complications. Key Word: Alcoholic liver disease, Ferritin, LFT markers, GGT, Oxidative stress
INTRODUCTION Alcoholic liver disease (ALD)includes wide range of clinical and morphological changes that range from fatty liver to hepatic inflammation and alcoholic hepatitis to progressive cirrhosis.1 Alcoholism is a serious health issue with socioeconomic consequences .The chronic consumption of alcohol causes multiple structural and functional derangements.2Alcohol at low doses is beneficial in decreasing the incidence of myocardial infarction, stroke, and alzheimer’s disease, but consumption more than two standard drinks-per day increases the risk of healthproblems.3Harmful effects of alcohol are encountered with regular consumption of 7.5 units (60 g) of alcohol per day in men and5 units (40g) per day in women.4The identification of alcoholics, especially in the early stages of alcohol abuse is important in preventing adverse health effects and socioeconomic consequences. Many biochemical parameters in blood and urine have been proposed as the biomarkers of alcoholism. The major biomarkers include alanine amino transferase (ALT), aspartate aminotransferase (AST), γ-glutamyl transferase (GGT), and carbohydrate deficient transferrin and many more. Iron plays an important role in various essential cell functions. However, excess iron is toxic and causes lipid peroxidation and tissue damage. Its absorption and transport therefore needs to be tightly regulated. It is a known fact that iron stores are increased in alcoholics. Iron accumulation has been proved as one of the mechanisms involved in chronic liver disease. Both iron and alcohol can initiate free radical formation and produce oxidative stress within liver and hence fasten the progression toward cirrhosis.5 ,6 Ferritin is a positive acute-phase protein. High serum ferritin is found in a large spectrum of conditions including haemochromatosis, alcoholic liver disease etc... Serum ferritin is frequently reported to be elevated in chronic alcoholics. The liver contains much of the iron stored in the body, and any process that damage liver cells will release ferritin. It is also possible that liver damage may interfere with clearance of ferritin from the circulation. Liver injury due to oxidative stress causes hepatic endothelial cells to release ferritin into circulation. Ferritin may amplify the toxic effects of alcohol towards fibrosis and cirrhosis. The leakage of tissue ferritin which is an intracellular iron storage protein, causes increase in serum ferritin.7 Serum gamma glutamyl transferase (GGT), is often the first marker to be elevated in alcoholics. It increases in a dose-dependent manner in alcohol misuse. It is less sensitive in women than men. The enzyme may be released by hepatic cell injury or by induction following exposure to alcohol. Hepatocyte cholestasis and hepatocytedamage in alcoholic liver disease causes increase in GGT. It increases after five weeks of drinkingmore than 50 g per day. It usually increases to three times the upper reference limit, but will normalise within five weeks of abstinence. It has a half-life of 26days.8 Serum GGT levels rise in response to the acute hepatocellular damage. The levels are especially high in patients with severe alcoholic liver disease. These are more likely to be elevated in the regular rather than the episodic drinkers. The alanine transaminase (ALT) and aspartate transaminase (AST) levels are elevated in patients with viral hepatitis, toxic hepatitis, cholestasis, cirrhosis, liver carcinoma, and alcoholic liver disease. The serum AST and ALT levels are often raised in patients who are alcoholics although generally not to more than 2-4 times the upper limits of the normal range. An AST/ALT ratio which is > 1.5, strongly suggests an alcohol- induced damage to the liver, and a ratio which is > 2.0 confirms this diagnosis.2 Several studies have reported elevated serum ferritin, LFT and GGT levels in patients with ALD. There are not many studies in India which show association of alcohol with ferritin, although incidence of alcohol abuse is quite high in India compared to other developing countries. Hence, the present study was undertaken to evaluate the effects of alcoholic liver disease on the serum levels of ferritin, GGT and other liver function test markers. We also hypothesized that serum ferritin may be acting as a marker of acute phase reactant, reflecting the inflammatory status of patients of chronic alcohol abuse, rather than as a marker of iron overload.
AIMS AND OBJECTIVES: To estimate and compare the levels of Serum ferritin, LFT and GGT in alcoholics and non alcoholics.
MATERIALS AND METHODS This study was conducted in Medicine OPD and inpatients admitted in SNMC and HSK hospital, Navanagar, Bagalkot, over a period of 6 months. Serum levels of ferritin, LFT and GGT were estimated in 50 male alcoholic patients who are considered as cases and50 controls who are age and sex matched healthy non-alcoholic subjects. Study design was case control study. Detailed clinical history was taken regarding number of drinks, type of drink and duration of alcohol drinking. Inclusion criteria:
Exclusion criteria: patients with
Written informed consent was taken. Institutional ethical committee approval was taken before starting the study. A sample of 5 ml venous blood was collected under standard aseptic precautions. Sample was centrifuged to obtain clear serum. Serum ferritin was estimated by chemiluminescence method. LFT were measured spectrophotometrically using A25 Biosystems Autoanalyser. GGT was estimated by SZASZ method using semiautoanalyser 3300. Statistical Analysis: Data obtained was tabulated and analysed by applying appropriate statistical tests using SPSS package version 17. Results were expressed as mean ±SD. Comparison of variables between two groups performed with student t-test. The p value < 0.05 were considered statistically significant.
RESULTS Table 1 shows mean age in both the groups and it is statistically insignificant. We have compared liver function parameters like Total bilirubin, direct and indirect bilirubin, total proteins, albumin and globulin, and liver enzymes like ALT and AST in both cases and controls. Table 2 shows statistically significant increased total bilirubin levels in cases. Serum albumin, Globulin, ALT, AST, GGT and ferritin were significantly increased in cases when compared to controls with p<0.05as shown in tables 3,4,5 respectively. Table 1: Mean age in both the groups:
Table 2: Total bilirubin, direct and indirect bilirubin levels in both the groups:
Table 3: Total protein, albumin and globulin levels in both the groups:
Table 4: SGOT, SGPT and ALP levels in cases and controls:
Table 5: Comparison of serum GGT and Ferritin levels in cases and controls:
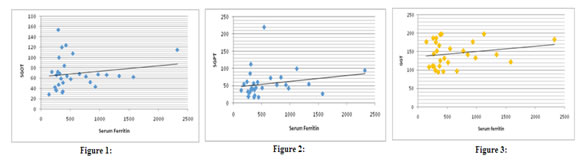
The levels of SGOT, SGPT and GGT showed positive correlation with serum ferritin levels but did not show statistical significance (fig 1,2,3). Figure 1: Pearson correlation of SGOT and ferritin; Figure 2: Pearson correlation of SGPT and ferritin; Figure 3: Pearson correlation of GGT and ferritin Table 6: Pearson’s Correlation between Ferritin with SGOT, SGPT and GGT in cases
DISCUSSION Our study provides striking evidence that alcohol consumption has effects on iron status. Increase in serum iron and ferritin may be useful in individuals who are iron deficient but not in all patients. Excess iron may lead to oxidative stress and generation of free radicals and may lead to harmful effects on liver. Our aim in this study was to show serum ferritin as oxidative stress marker. That is why we had excluded patients who were taking iron therapy, who had history of bleeding in the recent past and persons with other inflammations and infections. Alcoholic liver disease is commonly associated with iron overload. The possible mechanisms explained for iron overload are, taking iron in hepatocytes in specific way through increased levels of transferrin receptor (TfR) and increased intestinal iron absorption from decreasing hepcidin.9 The results explain that concentrations of Ferritin and GGT in the serum of alcoholics are significantly higher when compared with non alcoholics (p < 0.05)This is in accordance with studies by Suneetha N et al,T.E.Meyer et al, J. B. Whitfield et al.7,10,11 Total bilirubin, Serum albumin, Globulin, SGOT, SGPT, GGT and ferritin were significantly increased in cases when compared to controls with p<0.05.similar findings were obtained in other studies.12,13,14 The levels of SGOT and SGPT, GGT showed positive correlation with serum ferritin levels but did not show statistical significance. Alcohol consumption causes changes in oxidant-antioxidant system. Alcohol metabolism generates reactive oxygen species and lipid peroxidation products. Due to liver injury, hepatic endothelial cells release ferritin into circulation, in response to increased oxidative stress. Alcohol-mediated oxidative stress is involved in the inhibition ofhepcidin promoter activity and transcription in the liver. The combination of both agents may add up to exacerbate oxidativeinjury and fibrogenesis in the liver. It is possible that the elevations in serum markers of iron stores that we observed among alcohol users do not reflect a true elevation in body iron stores. It is also possible that alcohol consumption itself provokes changes in acute-phase proteins, of which ferritin is one.15
CONCLUSION In our study we found that serum ferritin is significantly increased in alcoholics. Serum ferritin may be acting as a marker of acute phase reactant, reflecting the inflammatory status of patients of alcohol abuse. Serum ferritin can be considered as an early marker of oxidative stress in alcoholics. Early detection and supplementation with antioxidants might delay the onset of cirrhosis. The current study provides evidence that serum ferritin may be a simple and useful adjunctive marker to clinicians in evaluation of patients with alcoholic liver disease. Limitations of the study: Our study is limited by the lack of data on mutations in the hemochromatosis gene (HFE), which can cause iron overload. We described iron overload or iron deficiency based entirely on serum ferritin, other iron markers were not estimated. We did not consider subclinical inflammation in subjects.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.