 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 1 - October 2019
Serum ferritin in pre-diabetes and diabetes mellitus in relationship with glycemic status
Sujatha Pasula1, Vamsi Krishna Chittimoju2*
1Assistant Professor, Department of Biochemistry, Osmania Medical college, Koti, Hyderabad, Telangana. 2Assistant Professor, Gayatri Vidya Parishad Institute of Healthcare and Medical Technology, Visakhapatnam, Andhra Pradesh. Email: vamsikrishna.b10@gmail.com
Abstract Background: Iron has been suggested to play a role in the etiology of type 2 diabetes mellitus (T2DM). Evidence are sparse for other markers of iron metabolism that are regulated differently and might act through independent pathways. Aims: To analyze the serum ferritin levels in individuals having diabetes and to study its association Glycated hemoglobin (HbA1c%). Materials and Methods: The present crosssectional study was conducted for a period of 15 months in 150 individuals: Group-1: 75 healthy subjects, and group-2: 75 patients diagnosed with type 2 Diabetes Mellitus Number of age and gender matched controls selected randomly. All the relevant demographic data were collected and anthropometric measurements including height and weight were measured to calculate BMI. Serum Ferritin levels in Type 2 diabetes mellitus and correlation between Serum ferritin and HbA1c% is done. Results: The highest prevalence was found in the age group 41-50 years (38%) followed by the age group of 51-60 (27%). It was observed that male female ratio of 1.2:1. Serum ferritin was significantly higher in the cases (p<0.01) when compared to controls. Serum ferritin was significantly related to the duration of diabetes (p<0.05). As the duration of diabetes increased, serum ferritin also increased. There was a positive correlation between serum ferritin and HbA1c. Serum ferritin is also significantly related to HbA1c (r- 0.21, p<0.05). Conclusion: serum ferritin was increased with HbA1c which is positively correlated in diabetes. Thus, routine screening for serum ferritin concentration in diabetic patients can be done to assess the body iron stores. Key Words: Glycated Hemoglobin, Ferritin, Insulin resistance.
INTRODUCTION Diabetes mellitus (DM), one of the most prevalent endocrine disorders in the India now reached the proportions of a global pandemic. India, has a very high number of diabetics and has earned rank of being the diabetes capital of the world. The earliest evidence that systemic iron overload could contribute to abnormal glucose metabolism was that patients with classic hereditary hemochromatosis (HH) had increased frequency of diabetes mellitus.1 Iron is an essential micronutrient for humans, primarily responsible for oxygen transport, electron transfer reactions and DNA synthesis. However, iron is also known to take part in the formation of highly reactive free radicals that can induce oxidative modification of various molecules (1). Since patients suffering from hereditary hemochromatosis – a disease characterized by massive iron overload – have been described to be more likely to develop type 2 diabetes mellitus (T2DM), iron overload is suspected to play a role in its etiology. Subsequent studies also suggested that elevated body iron stores, mainly measured by circulating ferritin levels, are associated with a higher T2DM risk in the general population. There is evidence that high body iron may have detrimental effects on both insulin secretion and sensitivity. However, more recent studies on diabetes in hereditary hemochromatosis have been inconclusive and ferritin levels may be influenced by reverse causation or confounding by inflammation, as ferritin is an acute-phase protein .2,3 Studies examined the relationship between ferritin and hyperglycemia or insulin resistance in humans. These studies in general found positive associations, although transferrin is inversely related to body iron stores and ferritin. In addition, while increased ferritin is quite consistently associated with hyperglycemia or insulin resistance.4 To analyze the serum ferritin levels in individuals having diabetes and to study its association Glycated hemoglobin (HbA1c%).
MATERIALS AND METHODS The present crosssectional study was conducted for a period of 15 months in the Department of Biochemistry. Out of a total of 150 individuals: Group-1: 75 healthy subjects, and group-2: 75 patients diagnosed with type 2 Diabetes Mellitus Number of age and gender matched controls selected randomly. All the relevant demographic data were collected and anthropometric measurements including height and weight were measured to calculate BMI. Under all aseptic and antiseptic conditions 5 ml of blood sample was collected from each subject from a suitable peripheral vein (preferably antecubital vein) by venipuncture using a sterile disposable syringe and divided into a sterile empty vial and an EDTA vial. EDTA vials are used for estimation of glycated hemoglobin. The rest of the sample was then allowed to stand for some time and then centrifuged for separation of serum. This serum was used for estimation of the other parameters. Serum ferritin was measured by immunoradiometric assay kit of the sandwich type based on two monoclonal antiferritin antibodies: one 125I- labelled anti-ferritin antibody in liquid phase and other monoclonal antiferritin antibody is coupled to magnetizable cellulose. Blood glucose was determined by the Hexokinase method and glycosylated hemoglobin by D 10 by HPLC method. Patients were evaluated with detailed history, meticulous examination and laboratory investigations. Since serum ferritin is an acute phase reactant and may be elevated in presence of inflammation, an attempt was made to minimize this potential source of confounding by excluding those patients with suspected infection, inflammation and liver disease and with positive CRP levels. Most of the patients were selected when they had come for treatment for diabetes. Statistical analysis Statistical analysis was performed using the software SPSS. Means of the different parameters were compared using one way analysis of variance (ANOV A). Pearson’s Correlations between serum ferritin, blood glucose and BMI were evaluated using Pearson Co-relation Co-efficient. All tests were considered statistically significant if the p-value was <0.05.
RESULTS In the present study carried out in diagnosed cases of type 2 diabetic mellitus, the youngest case study was found to be 33 years of age, and the oldest to be 75 years. The highest prevalence was found in the age group 41-50 years (38%) followed by the age group of 51-60 (27%). It was observed that male female ratio of 1.2:1.
Table 1: Comparison of Demographic details
Age, blood urea and serum creatinine are not significant on comparison in 2 groups. BMI, fasting blood glucose and post prandial blood glucose are significant in between the groups.
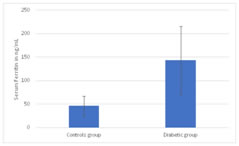
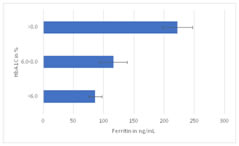
Figure 1 Figure 2 Figure 1: Serum ferritin in diabetic patients when compared to controls; Figure 2: Correlation between serum ferritin and HbA1c Figure 1, Serum ferritin was significantly higher in the cases (p<0.01) when compared to controls. Serum ferritin was significantly related to the duration of diabetes (p<0.05). Figure 2, As the duration of diabetes increased, serum ferritin also increased. There was a positive correlation between serum ferritin and HbA1c. Serum ferritin is also significantly related to HbA1c (r- 0.21, p<0.05). DISCUSSION CONCLUSION REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.