 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 - November 2019
Evaluation of vitamin d levels and seasonal variations among known population: An institutional based study
Anil Kumar1*, Sangeeta Kapoor2, Anjali Verma3, Sushil Yadav4
1Associate Professor, 2Professor and Head, 4Assistant Professor, Department of Biochemistry, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, INDIA. 3Associate Professor, Department of Physiology, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, INDIA. Email: dr.netin@gmail.com
Abstract Background: Vitamin D insufficiency and its implications has been a topic of intense debate among health professionals for many years; in fact, low vitamin D status in relation to major non-communicable diseases has been investigated in numerous observational studies. Hence; the present study was undertaken for assessing the seasonal variation occurring in vitamin D levels. Materials and Methods: A total of 200 patients were recruited who came for routine medical checkup. Group A: Patients in which vitamin D levels were assessed at the end of summer season, and Group B: Patients in which vitamin D levels were assessed at the end of winter season. There were 100 patients in each group. All the patients were called in the morning time. Fresh blood samples were obtained from all the patients. All the blood samples were sent to laboratory where an auto-analyzer was used for assessing the serum vitamin D levels. Results: Mean Vitamin D levels among patients at the end of summer season were 29.1 nmol/L, while mean vitamin D levels among patients at the end of winter season was 26.7 nmol/L. A significant reduction in vitamin D levels was among patients at the end of winter season especially among males. Conclusion: Due to inadequate sunlight in winters, there is comparatively higher deficiency of vitamin D among subject especially among females. Key Word: Sunlight, Vitamin D.
INTRODUCTION Vitamin D insufficiency and its implications has been a topic of intense debate among health professionals for many years; in fact, low vitamin D status in relation to major non-communicable diseases has been investigated in numerous observational studies. The main source of Vitamin D comes from sun exposure of the skin, from 7-dehidrocholesterol in response to ultraviolet B radiation (UVB), to further be metabolized in the liver to 25-hydroxyvitamin D 25(OH)D which is the metabolite used to assess vitamin D status.1- 3 It requires further metabolism by the 1-alpha hydroxylase (CYP27B1) in the kidneys to produce the biologically active form 1,25-dihydroxyvitamin D (1,25(OH)2D3). Solar radiation is weaker and hours of sunlight are shorter in winter compared with summer as well as in high latitudes compared with low latitudes. Thus, there is not only a higher prevalence of hypovitaminosis D compared with regions closer to the equator, but also a large seasonal variation, with higher levels at the end of summer and lower levels at the end of winter.4-6 Hence; the present study was undertaken for assessing the seasonal variation occurring in vitamin D levels.
MATERIALS AND METHODS The present study was conducted with the aim of assessing the seasonal variation occurring in vitamin D levels. Ethical approval was obtained from institutional ethical committee and written consent was obtained from all the patients after explaining in detail the entire research protocol. A total of 200 patients were recruited who came for routine medical checkup. Group A: Patients in which vitamin D levels were assessed at the end of summer season, and Group B: Patients in which vitamin D levels were assessed at the end of winter season. There were 100 patients in each group. All the patients were called in the morning time. Fresh blood samples were obtained from all the patients. All the blood samples were sent to laboratory where an auto-analyzer was used for assessing the serum vitamin D levels. All the results were recorded in Microsoft excel sheet and were analyzed by SPSS software. Chi- square test was sued for assessment of level of significance.
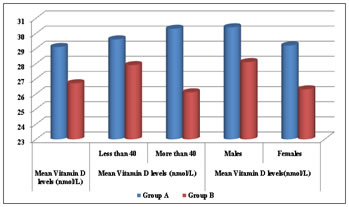
RESULTS Group A: Patients in which vitamin D levels were assessed at the end of summer season, and Group B: Patients in which vitamin D levels were assessed at the end of winter season. There were 100 patients in each group. Among group A, there were 39 males and 61 females while in group B there were 42 males and 58 females respectively. Mean Vitamin D levels among patients at the end of summer season were 29.1 nmol/L, while mean vitamin D levels among patients at the end of winter season was 26.7 nmol/L. A significant reduction in vitamin D levels was among patients at the end of winter season especially among males.
Table 1: Demographic data
Table 2: Mean Vitamin D levels among patients during summers and winters
Figure 2: Mean Vitamin D levels among patients during summers and winters
DISCUSSION Some studies have found that vitamin D levels increase in summer and decrease in winter due to dependency of vitamin D on sunlight. Studies have also shown that this seasonal variation might depend on latitude, since it has been found that vitamin D production is greater on latitudes close to the equator. However, vitamin D deficiency has even been reported in sunny regions.7- 9 This deficiency has been linked to many factors. For instance, skin pigmentation has a strong effect on vitamin D status, since it reduces the UVB radiation that effectively reaches the skin. In the same way, sunscreen use decreases vitamin D production. On the other hand, obesity is a risk factor. It has been proposed that this is due to fatty tissue uptake of vitamin D, reducing its bioavailability. BMI and WC in particular have been negatively associated with vitamin D levels and greater prevalence of deficiency. Regarding age, it has been proposed that vitamin D deficiency in the elderly can be attributed to a decrease in the skin capacity to produce vitamin D due to ageing, from a lack of exposure to sunlight, or from a deficient dietary intake.9, 10 In the present study, following two groups were recruited; Group A: Patients in which vitamin D levels were assessed at the end of summer season, and Group B: Patients in which vitamin D levels were assessed at the end of winter season. There were 100 patients in each group. Among group A, there were 39 males and 61 females while in group B there were 42 males and 58 females respectively. Niculescu DA et al assessed the seasonal variation of 25-hydroxy vitamin D [25(OH)D] in Romanian population. The 25(OH)D was measured by two different chemiluminescence or electrochemiluminescence assays. There were 8024 subjects (median age 50 (37, 62); 1429 men (17.8%)) without a diagnosis of low bone mass (osteopenia or osteoporosis). Serum 25(OH)D showed a marked seasonal variation with highest levels in September (24.1 18.3, 30.3] ng/mL) and lowest levels in March (13.5 [9.4, 19.6] ng/mL) (p < 0.001). The seasonal variation (early autumn vs. early spring) persisted in all age and sex groups and was maximal for 21-40 years of age (26.5 (20.8, 33.1) vs. 12.9 (9.7, 17.9) ng/mL) and minimal for >65 years of age (18.6 (13.0, 27.2) vs. 12.7 (7.8, 19.7) ng/mL). Men and women showed similar amplitude of serum 25(OH)D variation. The prevalence of vitamin D deficiency is high, particularly in the elderly. The data showed a strong seasonal variation of serum 25(OH)D in all subgroups of their Romanian population with highest levels in September and lowest levels in March.10 In the present study, Mean Vitamin D levels among patients at the end of summer season were 29.1 nmol/L, while mean vitamin D levels among patients at the end of winter season was 26.7 nmol/L. A significant reduction in vitamin D levels was among patients at the end of winter season especially among males. Al Zarooni AAA et al explored the prevalence of vitamin D deficiency, its seasonal variation and associated comorbidities among the Abu Dhabi Emirati population living in urban and suburban settings. Of the 12,346 participants 36.9% were male and 63.1% female. The majority (72%) were either vitamin D deficient (< 50 nmol/L), or (10%) vitamin D insufficient (50–74 nmol/L). Vitamin D deficiency was similar in both sexes (male 83.1% vs female 83.8%) as insufficiency (male 12.7% vs female 11.2%). Low vitamin D levels were associated with high blood pressure, high body mass index, central obesity, high cholesterol, impaired blood glucose levels and a high Framingham risk score. The mean vitamin D level was highest in January (winter) and lowest in July (summer).11 In winter time, due to the fact that there is inadequate sunlight, increased pollution and the factor of being 32° N, it leads to inadequate production of vitamin D in the skin, vitamin D levels are very low during winter.12
CONCLUSION From the above results, the authors conclude that due to inadequate sunlight in winters, there is comparatively higher deficiency of vitamin D among subject especially among females.
REFERENCES
|
||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.