 Home
Home
|
Table of Content - Volume 13 Issue 1 - January 2020
Study on the biochemistry laboratory performance in notifying critical alerts
J Sowndharya1*, S Aruna2, G Jeyachandran3
1Tutor, 2Assistant Professor, Department of Biochemistry, Government Karur Medical College and Hospital, Karur. 3Professor and HOD, Department of Biochemistry, PSG Institute of Medical Sciences and Research, Coimbatore. Email: sowndaryaj27@gmail.com
Abstract Background: Critical alert interval is the interval of examination (test) results that indicates an immediate risk to the patient of injury or death. Materials and Methods: All consecutive critical data of the month January 2019 are taken from the critical alert register from a tertiary care hospital/DC/BC/Reg/RR/09-Critical. From LIS, we generated the list of data satisfying the critical alert conditions in the same period January 2019. Results: The distribution had two peaks. The first peak is the tallest i.e.171 alerts are given within 25minutes. ABG and electrolyte samples processed immediately, contribute to this. This peak is superimposed on a normal distribution with a peak at 50 to 75 minutes interval and a long tail on the right side. Conclusion: Critical alert recording is missed in 26.3% of total alerts triggered. After correction, 50% of beta HCG is not recorded in the register. In 171 instances only we have given the alert within 25minutes. Key Words: Critical alert, Parameters, Samples, Notification and authorized personnel.
INTRODUCTION Critical alert interval is the interval of examination (test) results that indicates an immediate risk to the patient of injury or death. When examination results fall within established “alert” or “critical” intervals: -A physician (or other authorized health professional) is notified immediately. -Records are maintained of actions taken that document date, time, responsible laboratory staff member, person notified and examination results conveyed, and any difficulties encountered in notifications. This study is about how effectively it is practiced in the laboratory
MATERIALS AND METHODS Institutional human ethics committee approval was obtained. All consecutive critical data of the month January 2019 are taken from the critical alert register from a tertiary care hospital/DC/BC/Reg/RR/09-Critical. From LIS, we generated the list of data satisfying the critical alert conditions in the same period January 2019.
FOLLOW UP
Following are the parameters and their critical alert levels:
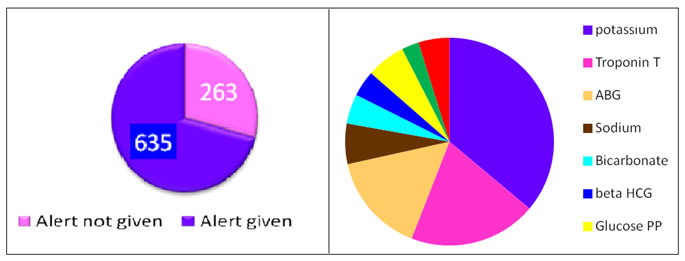
OBSERVATION AND RESULTS Figure A: Alerts recorded and not recorded Figure B: Parameter wise alert
Missed alerts compared with total alerts
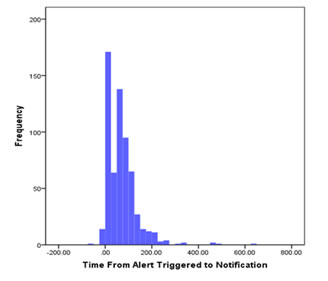
Time duration from alert triggered to alert notification
RESULTS The distribution had two peaks. The first peak is the tallest i.e.171 alerts are given within 25minutes. ABG and electrolyte samples processed immediately, contribute to this. This peak is superimposed on a normal distribution with a peak at 50 to 75 minutes interval and a long tail on the right side.
CONCLUSION Critical alert recording is missed in 26.3% of total alerts triggered. After correction, 50% of beta HCG is not recorded in the register. In 171 instances only we have given the alert within 25minutes. In 442 instances it took 26mts to 4hrs. In 12 samples, it took more than 4 hours.
REFERENCES
Policy for Articles with Open Access |
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.