 Home
Home
|
Table of Content - Volume 13 Issue 1 - January 2020
Study on correlation between glycated haemoglobin and serum lipid profile in type 2 diabetes mellitus
Romy W Marshnil1, Aaron Vetha Jose J2*
1,2Assistant Professor, Department of Biochemistry, Government Kanyakumari Medical College, Asaripallam, Nagercoil, Tamil Nadu, INDIA. Email: avjose@gmail.com
Abstract Background: Diabetes Mellitus is the most common endocrine disease leading on to long term complications involving eyes, kidneys, nerves and blood vessels. Lipid abnormality is one of the major contributory factor increasing the risk of development of cardiovascular disease in type-2 Diabetes Mellitus. This study was undertaken to look for the correlation between glycated haemoglobin (HbA1c) and serum Lipid profile parameters in type-2 Diabetes Mellitus. Aim: To study the correlation between glycated haemoglobin (HbA1c) and serum lipid profile levels in type-2 Diabetes Mellitus. Materials and Methods: The study group consisted of 150 patients with type-2 Diabetes Mellitus and 150 normal healthy people without Diabetes of age (40-70) years. Both fasting and post prandial blood samples were collected and the blood samples were used for fasting blood sugar, post prandial blood sugar, HbA1c and serum lipid profile analysis. Pearson’s correlation coefficient was used to find out the correlation between HbA1c and serum Lipid profile in type-2 Diabetes Mellitus. Results: There was a statistically significant increase in the mean HbA1C values in the Diabetic group when compared to the non-diabetic group (P<0.01), whereas, a statistically significant increase was observed in the levels of serum Total cholesterol, TGL, LDL and VLDL cholesterol. There was a statistically significant decrease in serum HDL cholesterol levels in the Diabetic group when compared to the healthy non-Diabetic group (P<0.01). There was a statistically significant positive correlation (P-value=0.00) between HbA1c and serum Total cholesterol, TGL, LDL and VLDL cholesterol in type 2 Diabetic patients. Also, there was a statistically significant negative correlation (r= -0.30,P-value=0.00) between HbA1c and serum HDL cholesterol in type 2 Diabetic patients. Conclusion: Dyslipidemia is commonly observed in type 2 Diabetes Mellitus patients with poor glycemic control. Key Words: Correlation, Glycated Haemoglobin (HbA1c), Lipid profile, Type-2 Diabetes Mellitus
INTRODUCTION WHO consultation report defines ‘Diabetes Mellitus’ as a metabolic disorder of multiple etiology characterized by chronic hyperglycemia with defects in carbohydrate, fat and protein metabolism resulting from defective Insulin secretion, Insulin action or both.1 The number of diabetic patients worldwide is estimated to be around 150 million, two-thirds of these people belong to developing countries. India alone accounts for 20 million diabetic subjects.2 The long term effects of Diabetes Mellitus include progressive development of specific complications of retinopathy with potential blindness, nephropathy leading to renal failure, risk of foot ulcer and features of autonomic dysfunction including sexual dysfunction.3 Of all the complications caused by Diabetes Mellitus, the most dangerous and life threatening one is the coronary artery disease (CAD). Diabetic patients have more than two-fold higher risk of developing coronary artery disease compared to non-diabetic subjects.4 As hyperglycaemia is strongly associated with the development and progression of diabetic complications, the need for accurate monitoring of blood glucose levels in diabetes is essential. It has been known since the early 1970’s that glucose can attach to many proteins, and one such protein is haemoglobin.5 The non-enzymatic addition of a sugar residue to the amino group of proteins is called glycation. Glycated haemoglobin (HbA1c) is formed by the addition of glucose to the N-terminal valine residue of the β-chain of haemoglobin. HbA1c constitutes 60-80% of the total glycated haemoglobin. HbA1c is formed within the red-blood cells at a rate directly proportional to the blood glucose concentrations and reflects the mean blood glucose levels over the previous six to eight weeks.6 The measurement of glycated haemoglobin, especially HbA1c is effective in monitoring long-term blood glucose control in people with Diabetes Mellitus. It provides a retrospective index of integrated plasma glucose values over an extended period of time and is unaffected by recent food intake or recent changes in blood sugar levels. Lipid abnormality is one of the major contributory factor for the increased risk of development of cardiovascular disease in diabetes.7 Hypertriglyceridemia, increased serum cholesterol and increased levels of LDL lipoproteins have been reported in diabetics.8 Among these abnormalities hypertriglyceridemia is the most common and is caused by a defective clearance of triglycerides.9 The enzymes lipoprotein lipase and hormone sensitive lipase which are essential for clearance of lipoproteins are found to have decreased activity in Insulin Dependent Diabetes Mellitus (IDDM) and mildly decreased activity in Non-Insulin Dependent Diabetes Mellitus (NIDDM).10,11 Hence control of blood glucose levels is vital in Diabetes Mellitus and HbA1c is a preferred index of long-term control of blood glucose. The present study was undertaken to look for the correlation between glycated haemoglobin (HbA1C) and serum lipid profile parameters in Diabetes mellitus.
MATERIALS AND METHODS This study is a case control study which was carried out in 150 people with type-2 Diabetes Mellitus and 150 normal healthy people without Diabetes visiting the Department of Medicine of Sree Mookambika Institute of Medical Sciences Hospital, Kulasekharam. The age group of the study subjects were (40-70) years. Ethical approval was obtained from the Institutional Ethical Committee and an informed consent was obtained from all the participants of the study. Blood samples collected from the study participants were assayed for fasting blood sugar, post prandial blood sugar, HbA1c and serum lipid profile determination using Beckmann Coulters Au480 fully automated analyser and Erba Transasia’s Chem 5 plus semi autoanalyser in the Clinical Biochemistry Laboratory of SreeMookambika Institute of Medical Sciences. HbA1c percentage was analysed by cation-exchange resin method using Glyco Haemoglobin reagent kit. Serum lipid profile levels were analysed by enzymatic kit methods. Statistical method of analysis Statistical analysis was done using SPSS statistical package version 21. Results were expressed in terms of Mean ± SD. Unpaired student’s t-test was used to compare the results between the diabetic and non-diabetic group. Pearson’s correlation coefficient was used to find out the correlation between serum lipid profile levels with HbA1c levels in type-2 Diabetic patients. Statistically significant variation was considered when p value was less than 0.05.
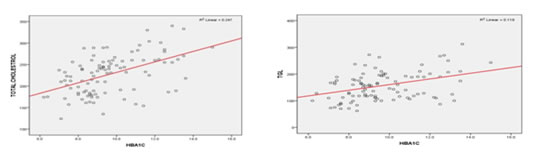
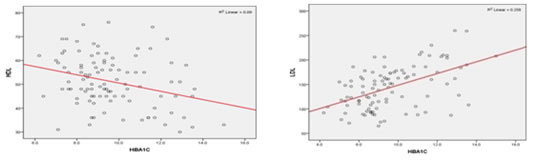
RESULTS A significant positive correlation was observed between HbA1c and serum total cholesterol (r=0.497), serum triglyceride (r= 0.344), serum LDL-cholesterol (r=0.508) and VLDL-cholesterol (r=0.344) levels in diabetic patients as seen in Fig (1.1, 1.2, 1.4 and1.5). There was a significant negative correlation (r=-0.300) between HbA1c and serum HDL-cholesterol levels in the diabetic patients as seen in Fig 1.3. Table I shows that, there is a statistically significant difference in the mean HbA1C values in the Diabetic group when compared to the non-diabetic group (P<0.01). Similarly, a statistically significant difference exists in the levels of Total cholesterol, TGL, HDL, LDL and VLDL in the Diabetic group when compared to the healthy group. The difference is found to be highly significant (P<0.01) for Total cholesterol, LDL and VLDL values in Diabetic patients when compared to controls. Table II evaluates the effect of known duration of Diabetes on glycated haemoglobin and serum lipid levels. From this table, it is seen that, there is a highly statistically significant effect of increased duration of diabetes on HbA1c, Total cholesterol and LDL Cholesterol levels (p<0.01). Also, there is a statistically significant increase in the TGL and VLDL Cholesterol levels (p<0.05) with increased duration of diabetes. From this table, it is also found that, there is no statistically significant effect of increased duration of diabetes on HDL cholesterol levels. Table III shows the effect of treatment with Oral hypoglycemics, Oral hypoglycemics and insulin, treatment with insulin alone on the levels of glycated hemoglobin and serum lipid levels in diabetic patients. From this Table it is seen that treatment showed highly statistically significant effects on the HbA1c, Total Cholesterol and LDL Cholesterol levels in Diabetic patients (P<0.01). Also, there is a statistically significant effect of treatment on TGL and VLDL Cholesterol levels in Diabetic patients (P<0.05). From this table it is found that there is no statistically significant effect of treatment on HDL Cholesterol levels (p>0.05). Fig 1.1: Total cholesterol andHbA1c Fig 1.2: TGL and HbA1c Fig 1.3: HDL andHbA1c Fig 1.4: LDL andHbA1c Fig 1.5: VLDL and HbA1c TABLE I: COMPARISON OF HbA1C AND LIPID LEVELS BETWEEN DIABETIC AND NON-DIABETIC
* Statistically significant –P Value<0.05 ** Statistically significant –P Value<0.01
TABLE II: EFFECT OF KNOWN DURATION OF DIABETES ON GLYCATED HEMOGLOBIN AND SERUM LIPID LEVELS
*Statistically significant - p Value < 0.05 **Statistically significant – p Value < 0.01 TABLE III: INFLUENCE OF TREATMENT ON THE LEVELS OF GLYCATED HEMOGLOBIN AND SERUM LIPID PROFILE IN DIABETIC PATIENTS
*Statistically significant - p Value < 0.05 **Statistically significant - p Value < 0.01 DISCUSSION In our study, the mean values of glycated haemoglobin in diabetic patients and non-diabetic controls were 9.64±1.86 and 5.51±0.31 respectively. This shows that, the mean values of glycated haemoglobin in diabetic patients were higher when compared to the non-diabetic controls. The increase was found to be highly statistically significant. Similar findings were also observed in another study done by Pasupathi P et al. 12 Results in our study (table-1) shows that, the mean values of serum Total cholesterol, serum Triglycerides, serum LDL- cholesterol and serum VLDL-cholesterol in the diabetic patients were 227.46± 67.52, 156.59±57.13, 144.13±43.62 and 31.23± 11.41 respectively. These values were higher than the mean values observed in non-diabetic healthy controls which were 186.20± 15.76, 135.32 ±19.44, 103.88± 17.49 and 26.80± 3.85 respectively. This increase was found to be statistically significant (p<0.05). Similar findings were observed in a study done by Samatha P. 13 In that study, the mean total cholesterol, triglyceride and LDL-cholesterol levels were increased in the diabetic patients when compared to the controls. Similar findings were also observed in studies done by IdogunES 14 and AlbrkiWM. 15 In this study, a significant positive correlation was observed between HbA1c and serum total cholesterol (r=0.497), serum triglyceride (r= 0.344), serum LDL-cholesterol (r=0.508) and VLDL-cholesterol (r=0.344) levels in diabetic patients. There was a significant negative correlation (r=-0.300) between HbA1c and serum HDL-cholesterol levels in the diabetic patients. These findings were in agreement with the study done by Khan HA. 16 Diabetic patients with elevated HbA1c and serum lipid values are considered very high-risk group for cardiovascular disease (CVD). Significant correlations between HbA1c and the lipid parameters and a linear relationship between HbA1c and dyslipidemia point towards the usefulness of HbA1c for screening high-risk diabetic patients. It has been estimated that reducing HbA1c levels by 0.2% could lower the cardiovascular risk by 10%. 17 In this study, longer duration of diabetes showed statistically significant effect on HbA1c, Total cholesterol, LDL-cholesterol, VLDL-cholesterol and TGL levels (p value <0.05). There was a highly statistically significant effect of longer duration of diabetes on HbA1c, Total cholesterol and LDL-cholesterol levels (p value<0.01). These findings were found to be similar to a study done by Rashid A and Haider I. 18 Effective treatment either with oral hypoglycemic agents or Insulin showed statistically significant effects on HbA1c, serum total cholesterol and LDL-cholesterol levels in diabetic patients. Diabetic care with diet and exercise modifications or medications have a great impact in lowering blood glucose levels, serum total cholesterol levels and LDL- cholesterol levels. 19 Micro vascular complications are reduced by 25% by effective diabetic treatment. There is a 35% reduction in risk of developing micro vascular complications with every 1% decrease in HbA1c levels.
CONCLUSION From the analysis of results obtained in type-2 diabetic patients and healthy age and sex matched controls without diabetes, the following conclusions were made:
REFERENCES
Policy for Articles with Open Access
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.