 Home
Home
|
Table of Content - Volume 14 Issue 3 - June 2020
A prospective study of hematological parameters among neonates with neonatal jaundice
Shailendra P Mosamkar
Tutor, Department of Biochemistry, K J Somaiya Medical College, Ayurvihar, Everad Nagar, Sion, Mumbai, Maharashtra, INDIA. Email: sathishkumard11@gmail.com
Abstract Background: Neonatal hyperbilirubinemia (NH) is commonest abnormal physical finding during the first week of life. Over two third of newborn babies develop clinical jaundice. The physical finding like yellowish discoloration of the skin and sclera in newborns is due to accumulation of unconjugated bilirubin. In most infants, unconjugated hyperbilirubinemia reflects a normal physiological phenomenon. Materials and Methods: A prospective cross sectional study on neonatal hyperbilirubinemia was conducted at one of the teaching institutes of K J Somaiya Medical College. Infants admitted with significant neonatal jaundice in first week of life are included in the study. Significant Jaundice was defined as total serum bilirubin exceeding 15mg/dl or even between 5 mg/dl and 15 mg/dl within 24 hour of birth or the same persisting beyond one week of life. Total 63 such cases of newborn were admitted during the study period of August 2019 to October 2019.Written informed consent were taken from the guardian of neonates. Detailed history of baby and mother was taken. Following investigations were done in all cases. Results: The present study includes 63 cases of newborn admitted in one of the tertiary care institutes. Various laboratory investigations of neonatal jaundice were carried out. Out of 63 neonates, almost two thirds (63.5%) were 2 to 3 days old. Mean age of the neonates was 2.97 days with standard deviation of 1.2 days. 37 (58.7%) were male while 26 (41.3%) were females. Percentage of Pre-term babies was 30.1. Neonates having low birth weight were 17 (26.9%).Conclusion: Neonatal hyperbilirubinemia is associated with various other clinical morbidities. Causes of hyperbilirubinemia should be investigated comprehensively. ABO and Rh typing should be done along with Coombs Test, reticulocyte count and G6PD screening. Key Words: Neonatal hyperbilirubinemia, clinical morbidities, Coombs Test, reticulocyte count and G6PD screening
INTRODUCTION Neonatal hyperbilirubinemia (NH) is commonest abnormal physical finding during the first week of life. Over two third of newborn babies develop clinical jaundice. The physical finding like yellowish discoloration of the skin and sclera in newborns is due to accumulation of unconjugated bilirubin. In most infants, unconjugated hyperbilirubinemia reflects a normal physiological phenomenon. NH nearly affects 60% of term and 80% of preterm neonates during first week of life. 6.1% of well term newborn have a serum bilirubin over 12.9 mg%. Serum bilirubin over 15 mg% is found in 3% of normal term newborns. Nevertheless untreated, severe unconjugated hyperbilirubinemia is potentially neurotoxic and conjugated hyperbilirubinemia is a harbinger of underlying serious illness. NH is a reflection of liver’s immature excretory pathway for bilirubin and is the most common reason for readmission of neonates in first week of life in current era of postnatal discharge from hospital3. Neonatal hyperbilirubinemia is a cause of concern for the parents as well as for the pediatricians. Premature babies have much higher incidence of neonatal jaundice requiring therapeutic intervention than term neonates. Hyperbilirubinemia was found to be the most common morbidity 65% among 137 extremely low birth weight neonates born over a period of 7 years in AIIMS. Elevated levels of unconjugated bilirubin can lead to bilirubin encephalopathy and subsequently kernicterus, with devastating, permanent neurodevelopment handicaps.6 Conjugated Hyperbilirubinemia indicates potentially serious hepatic disorders or systemic illnesses. Hence appropriate management of neonatal hyperbilirubinemia is of paramount importance. Hyperbilirubinemia can be treated either by phototherapy or exchange transfusion or pharmacologic agents. Phototherapy plays a significant role in prevention and treatment of hyperbilirubinemia. The main demonstrated value of phototherapy is that it reduces the need for exchange transfusion. As any treatment has its side effects, phototherapy also have its adverse effects like hyperthermia, feed intolerance, loose stools, skin rashes, bronze baby syndrome, retinal changes, dehydration, hypocalcemia, redistribution of blood flow and genotoxicity. Unlike other side effects, a very few studies are currently available that depicts the side effects of phototherapy on hematological parameters with controversial results. Hence the present study is undertaken to find out any significant changes in hematological parameters.
MATERIALS AND METHODS A prospective cross sectional study on neonatal hyperbilirubinemia was conducted at one of the teaching institutes of K J Somaiya Medical College. Infants admitted with significant neonatal jaundice in first week of life are included in the study. Significant Jaundice was defined as total serum bilirubin exceeding 15mg/dl or even between 5 mg/dl and 15 mg/dl within 24 hour of birth or the same persisting beyond one week of life. Total 63 such cases of newborn were admitted during the study period of August 2019 to October 2019.Written informed consent were taken from the guardian of neonates. Detailed history of baby and mother was taken. Following investigations were done in all cases. BLOOD GROUP (ABO/RH) OF MOTHER, FATHER AND BABY: The blood grouping was done by using known antisera with slide and tube methods SERUM BILIRUBIN ESTIMATION OF BABY: It has been done on auto analyzer by Diazo method of Pearlman and lee.
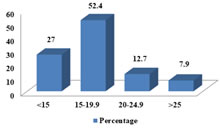
COMPLETE BLOOD COUNT WITH PERIPHERAL SMEAR EXAMINATION: It included haemoglobin, total count, different count, band cells, peripheral smear examination and reticulocyte count. DIRECT AND INDIRECT COOMB’S TEST OF BABY AND MOTHER RESPECTIVELY RETICULOCYTE COUNT: Reticulocytes count has been done by stain –Briliant cresyl blue. Test for G-6-PD deficiency has been carried out by using SPAN Diagnostic Reagent Kit from the red cell TEST FOR G-6-PD DEFICIENCY: hemolysate. C-REACTIVE PROTEIN OF BABY: has been carried out by Latex agglutination method Data was entered and analyzed by using appropriate statistical software. t test was used as a test of significance to find out the probability value. Study is approved by Ethical committee of Institution.RESULTS The present study includes 63 cases of newborn admitted in one of the tertiary care institutes. Various laboratory investigations of neonatal jaundice were carried out. Out of 63 neonates, almost two thirds (63.5%) were 2 to 3 days old. Mean age of the neonates was 2.97 days with standard deviation of 1.2 days. 37 (58.7%) were male while 26 (41.3%) were females. Percentage of Pre-term babies was 30.1. Neonates having low birth weight were 17 (26.9%). (Table 1) Physiological jaundice constituted (40) 62% cases of Neonatal hyperbilirubinemia. ABO incompatibility was the commonest cause of pathological jaundice and Septicemia is second commonest cause of pathological jaundice. (Table 2) Among half of the cases (33, 52.4%) range of serum total bilirubun was found between 15 and 19.9 mg/dl. 5(7.9%) were having the serum total bilirubin more than 25 mg/dl.(Figure 1) Hemoglobin level was lowest (12.1 gm %) in Rh incompatibility. Highest level of serum bilirubin was found in Rh Incompatibility whereas highest level of reticulocytes was noted in G-6PD Deficiency. Pre-term and low birth weight babies were having higher levels of serum total bilirubin but the difference was not significant (P>0.05) (Table 3) The rise in serum bilirubin level was found to be more in pathological jaundice as compare to physiological jaundice. Difference was significant statistically with p value of <0.05. (Table 4) Direct Coomb’s test and Indirect Coomb’s test were found to be positive in all case in Rh incompatibility while they were positive in 77% of cases in ABO incompatibility. (Table 5) In cases of septicemia CRP was found to be positive in 100% of cases. CRP was found to be positive in a few cases of ABO incompatibility (22.2%) and physiological jaundice (5%). (Table 6)
Table 1: Demographic profile of Neonatal Hyperbilirubinemia cases
Table 2: Etiology wise distribution of Neonatal Hyperbilirubinemia
Table 3: Mean level of Hemoglobin, Serum bilirubin and Reticulocyte count in Neonatal Hyperbilirubinemia
Table 4: Mean Serum bilirubin value: physiological Vs Pathological Neonatal Jaundice
Table 5: Result of Coomb’s test in Rh and ABO incompatibility
Table 6: Result of C-reactive protein in Neonatal Septicemia
Figure 1: Level of serum total bilirubin (mg/dl) among the neonatal jaundice cases
In present study, percentage of Pre-term (<37 weeks) babies was 30.1 and neonates having low birth weight (<2.5 kg) were 17(26.9%). In the study of Nepal D et al. LBW babies constituted 19.2%. Where as in the study of Choudhury Habibur Rasul 42% patients with neonatal jaundice had low birth weight and 37% were preterm. In our study out of 63, 40 (62%) cases were diagnosed as having physiological jaundice by while others were having ABO incompatibility (15%), Rh incompatibility (8%), septicemia (12%) and G-6 PD deficiency (3%). In the study of Nepal D et al. they noted that clinical sepsis as defined by WHO criteria was found in 86.3% of babies. Nearly 1/3rd (32.9%) babies were ABO incompatible and 4.1% babies were Rh incompatible. Choudhury Habibur Rasul et al. mentioned that Physiological jaundice was most common and was diagnosed in 114 (26.7%) cases. In their study Prematurity (20.9%) and sepsis (17.6%) were also major causes of jaundice. C. N. Onyearugha concluded in their study that septicaemia followed by prematurity were the leading aetiological factors of neonatal jaundice. Joshi et al. reported that in Septicemia, ABO incompatibility, Rh incompatibility were observed in 36.36%, 31.8%, 4.54% cases of neonatal jaundice respectively.G-6 PD deficiency was there in 3 percent of cases in present study. Singhal et al. reported almost similar finding (G-6 PD deficiency in 5% of cases) in their study. In present study mean Hb level was 14.2+/-1.7 gm/dl with range of 10-18gm/dl. Similar findings were noted in the study carried out by Joshi et al.. The findings of their study showed Mean Hb level of 13.87+/- 3.59gm/dl with a range of 8– 19.4 gm/dl.
CONCLUSION To conclude, most of the cases were having idiopathic jaundice although septicemia and ABO-Rh incompatibility were not exceptional. Peak serum bilirubin levels were found to be more among the pathological jaundice. Also prematurity and low birth weight were having higher levels of s. bilirubin. Special care must be given to them in order to avoid future complications of hyperbilirubinemia
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Anesthesiology (Print ISSN:2579-0900) (Online ISSN: 2636-4654) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.