 Home
Home
|
Table of Content - Volume 14 Issue 3 - June 2020
Study of mineral changes in patients with lung and breast cancer
Deepak P Birwatkar
1 Scientific Officer – D, Hematopathology, Hematopathology Laboratory. Tata Hospital, Annex Building, 5th floor, Parel, Mumbai, Maharashtra, INDIA. Email: drsarane@gmail.com
Abstract Background: Cancer is a leading cause of death worldwide and more than 70% of all cancer deaths occurred in low- and middle-income countries. Deaths from cancer worldwide are projected to continue rising, with an estimated 11.5 million deaths in 2030. Lung and Breast cancers are two main types of cancer in India. Material and Methods: The present study was comparative study carried out in patients suffering from lung and breast cancer and healthy subjects at department of biochemistry of KEM and Tata hospital, Mumbai. Sixty healthy and sixty cancer patients were enrolled in this study. Laboratory investigations were carried out to measure the serum levels calcium, phosphorus, zinc, copper and magnesium. The data collected from the analysis of serum were statistically analysed and evaluated for correlation between parameters and type of cancer. Results: In both lung cancer and breast cancer patients, serum calcium and serum phosphorus levels showed elevation in comparison to control group. Serum zinc levels remained elevated in lung cancer patients but showed reduction in female patients suffering from breast cancer. Serum copper levels remained elevated in all the groups of cancer patients except in male patients from lung cancer group. Serum magnesium remained elevated only in lung cancer patients. Positive correlation studied between calcium/phosphorus, calcium/magnesium and copper/zinc ratios in both groups of cancer patients. Conclusion: From the present study, it can be concluded that association of selected minerals under study with lung and breast cancer patients can be observed. A well planned and extensive large sample study will be required to confirm findings of the present study. Key Words: calcium, zinc, copper, phosphorus, magnesium, cancer, lung, breast.
INTRODUCTION The term “Cancer” is derived from the Greek word “Karkinos” (for crab) which refers to a generic non-communicable disease (NCD) characterized by growth of malignant (cancerous or neoplasms) abnormal cells (tumor/lump) in any part of the human body1,2. Although several forms of cancer have been detected, the most common sites of these tumors in human bodies are lungs, stomach, colorectal, liver, and breasts 3,4. With the ongoing demographic and epidemiological transition, cancer is emerging as a major public health concern in India. According to WHO, India has a cancer mortality rate of 79 per 100,000 deaths and accounts for over 6 percent of total deaths.5 These numbers are very close to those of high-income countries. Further, the cancer mortality in India is projected to increase by the end of this decade. According to GLOBOCAN data, top 5 cancers that affect Indian population are breast, oral, cervical, gastric and lung cancers. Trace elements are micronutrients that are part of daily diets, they are required in minute quantity, but are very important in many different biological processes, such as function of structural nutrients, normal healing, metabolism of genetic materials for growth and differentiation, programmed cell death and necrosis, protection against oxidative injuries and anti-inflammatory and anti-carcinogenesis effect. On the other hand, some are also involved in undesirable events in vivo, such as participation in carcinogenesis and sustenance of cancerous cells in which lead, copper; chromium and zinc have been implicated. Some of the specific desirable anti-carcinogenetic activities of trace elements include the role of selenium in prevention of oxidative stress through its activity in glutathione and super oxide dismutase and activation of p53 a tumor suppressor gene and the role of zinc in the application of brakes in the cell cycle and induction of apoptosis. The in vivo utilization of trace elements is complex and not completely understood. They have redundancy of function because the same element may incite both positive and negative events depending upon its concentration and interaction with other trace elements.6 The concentration of trace elements in body fluids and tissues are influenced by sex and age, the dietary intake, uptake in the gastrointestinal tract, storage, excretion and the presence or absence of disease state. These numerous influencing factors raise the question, of which is the appropriate tissue for estimating the bioactivity of these elements. However, for some of these elements, zinc, copper and selenium inclusive, the serum concentration has been found to be is a reliable measure of their bioactivity in the body, 7 Since indication of the possibility of the direct or indirect influence of trace element in the development and prevention of malignant diseases the contribution of the trace elements has been under scrutiny. Trace elements have been implicated in the pathogenesis of breast cancer.8 In various body tissues, varying concentrations and relationships have been documented world-wide. Inverse relationship has also been found between the concentration of zinc in the blood and presence of cancer of the breast while a direct relationship has been found between serum copper and copper-zinc ratio (C/Z) and cancer of the breast. 8,9 In India, approximately 63,000 new lung cancer cases are reported each year. The major risk factor for developing lung cancer is tobacco use and this disease is often viewed solely as a smoker's disease. However, a significant number of patients with lung cancer have no history of smoking. Although multiple risk factors, including environmental, hormonal, genetic and viral have been implicated in the pathogenesis of lung cancer in never-smokers, no distinct etiologic factor has emerged that can explain the relatively high incidence of lung cancer in never-smokers and the marked geographic differences in gender proportions. Apart from trace elements, minerals like calcium, phosphorous and magnesium role have also been studied in pathology of cancers. Due to the inconsistencies in the documentations on trace elements and some minerals in cancer of the breast and lung, we decided to determine the serum concentration of these in serum of female patients afflicted with breast cancer in comparison and serum concentration of female and male patients afflicted with lung cancer of study groups in comparison with healthy controls in our centre.
MATERIALS AND METHODS The present study was carried out in department of biochemistry of Seth GS Medical College and KEM Hospital, Mumbai and Tata Memorial Hospital, Mumbai. The study commenced after obtaining the sanction of the hospital ethics committee. Patients suffering cancer referred either from Tata or KEM Hospital were considered after confirming inclusion criteria. In this study, 60 patients suffering from cancer along with 60 normal healthy controls were evaluated. The study was carried out on newly diagnosed cancer patients and grouped them as given below; The study divided into following groups as follows;
Study plan: All these patients along with normal healthy controls were evaluated clinically and following laboratory investigations were carried out;
Blood samples collected by venepuncture, were allowed to clot at room temperature and serum was separated within 2 hours of withdrawal of blood and divided into aliquots which were stored at 40C until analysed. Instruments used for estimation were Spectronic 20 Spectrophotometer, Shimadzu’s UV- Spectrophotometer, Remi’s refrigerated centrifuge, ordinary centrifuge and vortex mixture. The data collected from the analysis of serum were statistically analysed and evaluated for association between parameters and type of cancer.
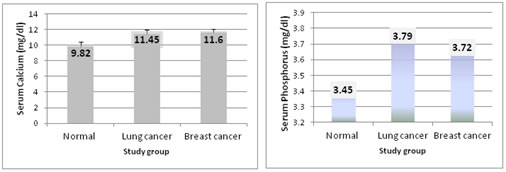
RESULTS The principle elements like calcium, phosphorus; magnesium and trace elements like zinc and copper were assessed in the serum samples and the variations observed in the groups have been summarized in a table below; Table 1: Variations in Serum level (mean ± SD) and range of parameters studied in different groups
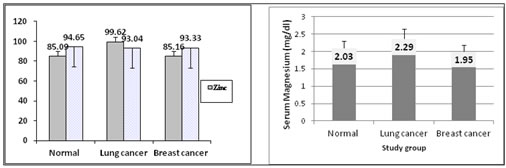
Graph 1: Variations in Serum Calcium levels different groups; Graph 2: Variations in Serum Phosphorus levels different groups Graph 3: Variations in Serum Zinc and Phosphorus levels in µg/dl different groups; Graph 4: Variations in Serum Magnesium levels different groups
Table 2: Variation in mean ± SD and percent mean variation of different parameters studied in Normal (Gp I) and patients suffering from Lung cancer (Gp II)
*: p<0.05 ; **: p<0.01 ; ***: p<0.001; NS : Not significant This table indicates increase in mean ± SD levels of all the parameters studied except for serum copper levels. The statistically significant increase in percentage is observed for calcium (p<0.001), phosphorus (p<0.01), zinc (p<0.001) and magnesium (p<0.001) respectively. Table 3: Variation in mean ± SD and percent mean variation of different parameters studied in Normal females (Gp I) and female patients suffering from Breast cancer (Gp III)
*: p<0.05 ; **: p<0.01 ; ***: p<0.001; NS : Not significant This table shows percentage increase in mean ± SD levels of calcium (118.37%), phosphorus (108.14%) and copper (102.11%) in breast cancer suffering female patients from Group III with respect to Normal group I subjects. The zinc and magnesium levels show insignificant decrease in mean ± SD.
Table 4: Gender wise differentiation (mean ± SD) and range in various parameters studied in different groups
Table 4 summarizes gender wise differentiation (mean ± SD) and range in various parameters studied in different groups.
Table 5: Variation in mean±SD and percent mean variation of different parameters studied in males from Normal (Gp I) (n= 29) and males from Lung cancer patients (Gp II) (n= 19)
*: p<0.05 ; **: p<0.01 ; ***: p<0.001; NS : Not significant Table 5 data indicates statistical increase in mean levels of all parameters except serum copper.
Table 6: Variation in mean±SD and percent mean variation of different parameters studied in females from Normal (Gp I) (n= 31) and females from Lung cancer patients (Gp III) (n= 11)
*: p<0.05 ; **: p<0.01 ; ***: p<0.001; NS : Not significant The above table indicates variations in mean levels of calcium, phosphorus, zinc and magnesium. The variation in copper level is insignificant. Calcium, zinc and magnesium levels indicate statistical increase (p<0.001), (p<0.001) and (p<0.01) respectively.
Table 7: Variation in mean±SD and percent mean variation of different parameters studied in females from Normal (Gp I) (n= 31) and females from Breast cancer patients (Gp III) (n= 30)
*: p<0.05 ; **: p<0.01 ; ***: p<0.001; NS : Not significant The table reveals statistically significant increase in calcium and phosphorus levels.
Table 8: Variations in Serum levels mean± SD and range of calcium/phosphorus, calcium/magnesium and copper/zinc ratios in different groups
Table 8 summarizes variations in Serum levels mean± SD and range of calcium/phosphorus, calcium/magnesium and copper/zinc ratios in different groups.
Table 9: Gender wise differentiation mean± SD and range of calcium/phosphorus, calcium/magnesium and copper/zinc ratios in different groups
Table 10: Variation in mean± SD and percent mean variation of calcium/phosphorus, calcium/magnesium and copper/zinc ratios in males and female patients with lung and breast cancer in comparison to normal subjects
Male patients in lung cancer group showed significant increase in the calcium/phosphorus and significant decrease copper/zinc ratio whereas female patients in lung cancer group showed statistically significant percent decrease in the copper/zinc ratio. Female patients in breast cancer group showed statistically significant percent increase in the calcium/phosphorus and calcium/ magnesium ratios. DISCUSSION The biologic and pathologic role of minerals and trace elements are numerous, complex and sometimes very inconsistent. Their role apparently depends on the concentration and the balance of the positively and negatively implicated elements among other factors. Because of the multiplicity of function and the varying role depending on balance and concentration, the role of these elements in the management of patients is yet to be fully elucidated. Breast cancer is the most common malignant tumor in females and a leading cause of malignant death in females. Its etiology is multi-factorial. Emphasis has been directed at trace elements as one of the modifiable risk factors.,10 Similar to other studies, our study shows that the serum concentration of copper, zinc differ between breast cancer bearing patients and healthy individuals. In our study, zinc levels showed marginal increase in lung cancer patients. Hypercalcemia is observed in both breast cancer and lung cancer patients. Lung cancer is the leading cause of cancer mortality worldwide and incurs the highest economic burden of all cancers. Lung cancer is a disease for which environmental factors (e.g., smoking, gender, asbestosis and pollution) play an important role. Besides smoking, emerging evidence also suggest that dietary factors may have an impact on the risk of lung cancer.11 To date, limited evidence exists on the role of dietary mineral intake, such as calcium, copper, iron, magnesium, selenium and zinc in the development of lung cancer. Copper, magnesium, selenium and zinc are essential dietary minerals for maintaining the integrity of DNA by preventing oxidative DNA damage.12 Evidence from in vitro and experimental studies suggests that DNA damage and defects in DNA repair mechanisms can predispose to cancer development. Likewise, epidemiological studies have shown that DNA repair capacity is associated with increased lung cancer risk.13 Calcium is another important mineral involved in processes of cell proliferation and carcinogenesis through cell signaling and cell cycle regulation. However, previous studies evaluating the relationship between dietary mineral intake and lung cancer risk have shown inconsistent results. Moreover, the most recent report from the World Cancer Research Fund concluded that current evidence is still insufficient to allow any dietary recommendations for calcium, copper, iron, magnesium, selenium and zinc to reduce the risk of lung cancer.11 The association between these minerals (dietary calcium, copper and magnesium) and lung cancer has been investigated in few prospective studies with conflicting results. Our finding of no association of dietary magnesium intake and breast cancer risk is in agreement with the results of two previous cohort studies; however, others described an increased risk of lung cancer in subgroup analyses. The relation between dietary copper intake and lung cancer risk has been rarely reported among cohort studies. Similar to our results, only one cohort study reported no association between dietary copper intake and lung cancer.4As documented by earlier researchers, the serum concentration of zinc in this study was significantly lower in breast cancer patients compared with healthy controls. This is in support of the finding of hypozincemia associated with the burden of breast cancer. The role of zinc as antioxidant defense is suspected to be the reason for its deficiency, whether this deficiency state precedes the disease or occurs in defense against the cancerous process is still undecided, it is however, suggested that a deficiency of zinc predisposes to chromosomal damage. Aside from the use of zinc as antioxidant, other factors that could be responsible for the hypozincemia in cancer patients are the increased loss in urine, the increased uptake of zinc by cancer cells and the presence other normal homeostatic control mechanisms and pathologic processes not related to the presence of the malignancy. Copper is a cofactor during redox reaction in cells. When in excess concentration however it binds to genetic material inducing oxidative damages. In support of previous studies, we found higher concentration of copper in blood of the breast carcinoma and lung cancer female patients compared to healthy matched adults. We also found higher copper zinc ratio in the cancer bearing patients. This relationship between copper and zinc is in concordance with earlier documentation. Even though, the exact mechanism responsible for the alterations in blood concentration of trace elements in cancer patients is yet to be fully understood, the findings in this study further lends credence to the presence of an inverse relationship between the negatively implicated element, copper and the positively implicated elements, zinc, in cancer bearing patients. 9,14 Our study results showed similarities with most of the observations of the previously published studies on copper and zinc levels. Exposure to trace metals and tissue concentration of trace element is a modifiable risk factor. Hence, discovery of a credible and strong causal association between trace elements and cancer of the breast and lung may create a new frontier for the attempt at prevention and for the overall management of an established disease.
CONCLUSION Limited data are available on the role of mineral intake in the development of lung and breast cancer. We investigated a possible link of dietary calcium, phosphorus, copper, magnesium and zinc intake with lung cancer and breast cancer risk. A well planned and extensive research will now be required to add the valuable information on the basic biochemical changes in minerals in these types of cancer patients.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.