 Home
Home
|
Table of Content - Volume 19 Issue 3 - September 2021
Serum uric acid and serum creatinine in sub-clinical and overt hypothyroidism - A case-control study
Amrut Arvindrao Dambal1, D Sridevi2*, Sidrah3, G Lakshmi Chaitanya4
1Professor & HOD, 2Professor, 4Assistant Professor, Department of Biochemistry, Malla Reddy Institute of Medical Sciences, Hyderabad, Telangana, INDIA. 3Tutor, Department of Biochemistry, Dr Patnam Mahender Reddy Institute of Medical Sciences, Rangareddy, Telangana, INDIA. Email: sridumedico81@gmail.com
Abstract Background: Thyroid gland is one of the largest endocrine glands in the body, which secretes thyroxine (T4) and triiodothyronine (T3). Thyroid hormones play a vital role in metabolic and physiologic homeostasis Few literatures have revealed that overt and subclinical hypothyroidism can be associated with increased risk of chronic kidney disease. Studies have revealed that serum creatinine and uric acid levels are marginally increased in hypothyroidism. Objectives: To understand the effect of subclinical hypothyroidism and overt hypothyroidism on serum creatinine and uric acid levels. Materials and Method: This case-control study was conducted in Malla Reddy Hospital, a teaching hospital associated with Malla Reddy Institute of Medical Sciences, Hyderabad taking 50 Subjects each who were identified with overt hypothyroidism and Sub Clinical Hypothyroidism as cases and 50 age and sex matched apparently normal healthy subjects from general population as controls. Estimation of Serum total T3, total T4, Thyroid Stimulating Hormone (TSH), Serum uric acid and serum creatinine were estimated for all the subjects. Results: It was observed that there was statistically significant increase in serum creatinine in subclinical hypothyroidism and both and serum creatinine and uric acid levels in overt hypothyroid subjects as compared to normal subjects. Conclusion: The present study indicates the influence of thyroid hormones on renal function. Therefore thyroid hormones have to be routinely assessed for patients presenting with deranged renal function. Keywords: Hypothyroidism, sub clinical hypothyroidism, Total Triiodothyronin (TT3), Total Thyroxin (TT4), Thyroid stimulating hormone (TSH)
INTRODUCTION Thyroid gland is one of the largest endocrine glands in the body, which secretes thyroxine (T4) and triiodothyronine (T3). Thyroid hormones plays a vital role in metabolic and physiologic homeostasis and regulate cardiac output, heart rate, ventilation rate, basal metabolic rate, effects of catecholamines, brain and metabolism of biochemical molecules like proteins, carbohydrates etc.1,2 Thyroid disorder is a progressive metabolic disorder which affects entire body functions and presents with various clinical conditions. Thyroid disease consequence have been found increasing day by day affecting all age groups in both male and females. The thyroid gland dysfunction may lead to chronic kidney diseases. Hypothyroidism is a clinical syndrome caused by the deficiency of thyroid hormones that cause a generalized slowing of metabolic processes3. Relationship between thyroid diseases and renal functions were initially considered as clinically insignificant and random, but few literature have revealed that overt and subclinical hypothyroidism can be associated with increased risk of chronic kidney disease 4,5,6Studies have revealed that serum creatinine and uric acid levels are marginally increased in hypothyroidism. The serum creatinine concentration increases in hypothyroid patients due to reduction of glomerular filtration rate because of hemodynamic changes in severe hypothyroidism7. In hypothyroidism the hyperuricemia is secondary to a decreased renal plasma flow and impaired glomerular filtration.8 Subclinical hypothyroidism (SCH), is an asymptomatic condition where peripheral thyroid hormone levels are within normal reference laboratory range but serum thyroid-stimulating hormone (TSH) level is mildly elevated. Very few studies were done regarding derangement of serum creatinine and uric acid levels in subclinical hypothyroidism. So a study was taken up to understand the effect of subclinical hypothyroidism and overt hypothyroidism on serum creatinine and uric acid levels.
MATERIAL AND METHODS This case-control study was conducted in Malla Reddy Hospital, a teaching hospital associated with Malla Reddy Institute of Medical Sciences, Hyderabad between August 2015 to June 2016. This study was taken up with 50 Subjects each who were identified with overt hypothyroidism and Sub Clinical Hypothyroidism as cases and 50 age and sex matched apparently normal healthy subjects from general population as controls. Inclusion criteria: The study includes all the subjects in the age group of 20–50 years of either sex attending the OPD in Malla Reddy Hospital, Hyderabad. The subjects were divided into three groups after laboratory investigations:
Cases Group 1: Sub Clinical Hypothyroidism: Asymptomatic subjects with serum TSH between 5.5 -10 μIU/ml and Total T3andT4 within the normal reference range • Group 2: Overt hypothyroid (OHT): Subjects having higher TSH and low Total T3andT4 and • Controls: Euthyroid subjects having TSH, Total T3 and T4 all within the normal reference range. Exclusion criteria: Patients with chronic kidney disease, gout, muscular dystrophies, patients on high protein diet, diabetes, hypertension, pregnancy, and patients on drugs for treatment of thyroid disorders or any other medications that might affect kidney functions are excluded from the study. Ethical Considerations: Ethical Clearance was obtained from the institutional ethics committee of the institution. Informed consent for involvement in the study and venipuncture was obtained from the subjects after explaining the objectives of the study in detail. Blood Sample Collection: Venous blood was drawn using a plain disposable vacutainer system in fasting state in aseptic condition. Serum was separated and analysis of biochemical parameters was done. Estimation of Serum total T3, total T4 and Thyroid Stimulating Hormone (TSH) were estimated by Monobind Acculite TSH kits using CLIA9. Serum Uric Acid was estimated by Uricase – Perioxidase method 10 and serum creatinine was estimated by modified Jaffe’s method using fully automated general chemistry analyser 11 Statistical Analysis: Comparison of the above biochemical parameters between cases and controls was conducted by student t test and expressed as Mean ± Standard Deviation. SPSS Package Version 20 statistical software was used to correlate the parameters p<0.05 and p <0.01 were considered as statistically significant and highly significant respectively.
RESULTS Table 1: Displaying number of subjects with gender and Mean age
Table 2: Comparison of Serum TT3, TT4, TSH, Serum Creatinine, Serum Uric acid among Controls and Hypothyroid Subjects
Table 3: Comparison of Serum TT3, TT4, TSH, Serum Creatinine, Serum Uric acid among Controls and Subclinical Hypothyroid Subjects
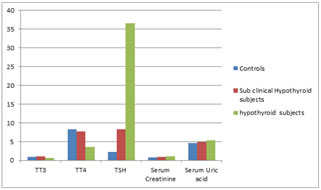
Figure 1: Comparison of Serum TT3, TT4, TSH, Serum Creatinine, Serum Uric acid among Controls and Subclinical Hypothyroid and Hypothyroid Subjects
This was a age and sex matched study with mean age among controls and two groups of cases being 48.12 ± 2.34, 46.41 ± 3.15and49.02 ± 2.07 (Table 1) As mentioned in Table 2, there was an extremely significant statistical difference between Group 1 and Group 2 for serum creatinine (p value<0.0001) and highly significant statistical difference between Group 1 and Group 2 for serum uric acid (p value < 0.001 ). As mentioned in Table 3, there was an extremely significant statistical difference between Group 1 and Group 3 for serum creatinine (p value < 0.0001) and unsignificant statistical difference between Group 1 and Group 3 for serum uric acid (p value = 0.05).
DISCUSSION This present study evaluated Serum creatinine and Serum uric acid levels in subclinical hypothyroid subjects and overt hypothyroid subjects in comparison with euthyroid controls. In this present study there was statistically significant increase in serum creatinine and uric acid levels in overt hypothyroid patients as compared to controls. Our study is in accordance with the studies done by Kreisman SH et al. and Nagarajappa K et al., Simbita et al., Md. Aminul haque Khan et al. where they observed that serum creatinine and Serum uric acid were significantly elevated in hypothyroidism.5,12,13,14 Thyroid dysfunction causes significant changes in kidney function and the most common kidney derangements associated with hypothyroidism are reduction in GFR and renal plasma flow.15 Sara Abdalseed Hamed study confirms that the hypothyroid state is associated with a consistent elevation in the serum creatinine level and reduced creatinine clearance, presumably due to a decrease in the GFR, and hyperthyroid state associated with increase in creatinine clearance compared with euthyroid control group.16 Sarika Arora et al. study showed that there is significant increase in creatinine levels (0.85}0.29) in overt hypothyroid subjects as compared to euthyroid subjects(0.71}0.27). These changes may result in physiological effects including alterations in renal hemodynamics, decrease in GFR and hence reduced clearance of creatinine.17Erickson et al. prospectively evaluated 54 patients with a documented gouty arthritis for the presence of hypothyroidism 18 .The prevalence of hypothyroidism was significantly higher in patients with gouty arthritis and he suggested screening for hypothyroidism should be considered in all patients presenting with gouty arthritis and those with a history of recurrent gouty flares. Giordano et al. studied 28 patients with primary hypothyroidism and found a significant increase in the incidence of both hyperuricaemia and gout in the hypothyroid patients8 They anticipated a possible interrelationship between purine nucleotide metabolism and thyroid endocrine disorders, in particular primary hypothyroidism and contemplated hypothyroid hyperuricemia is due to a reduction in renal plasma flow and glomerular filtration secondary to thyroid hormone deficiency. In a study done by Vijetha et al., it was observed that serum creatinine levels were significantly higher in the Sub Clinical Hypothyroidism group when compared to the control group.19
CONCLUSION The present study indicates the influence of thyroid hormones on renal function. This information may be necessary to avoid unnecessary investigations, cost and patient’s worry who presents with either increased creatinine or uric acid with undetermined thyroid status. Therefore, thyroid hormones have to be routinely assessed for patients presenting with deranged renal function. Routine evaluation of thyroid hormomes can be useful to avoid renal derangement in future and its management.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.