|
Table of Content - Volume 20 Issue 1 - October 2021
A review on diagnosis of lipid profile and non-alcoholic fatty liver disease with special emphasis to ultrasound based on Meta-analysis studies of western countries
Kavindra Kishanrao Borgaonkar1*, Ranjit Dattatraya Patil2, Lavanya Kaparti3, Pradeep Vaijanathrao Benjarge4
1Associate Professor, Department of Biochemistry, Vilasrao Deshmukh Government Medical College Latur 413512 Maharashtra, INDIA. 2Professor, Department of Medical Biochemistry, SSR Medical College Belle Rive, MAURITIUS. 3Associate Professor, Department of Anaesthesiology, Sri Devraj Urs Medical College, Tamaka, Kolar 563103 Karnataka, INDIA. 4Physician and Intensivist, Krishna hospital & ICU, Rokadiya hanuman colony Jalana road Aurangabad, Maharashtra, INDIA. Email: kb2172@rediffmail.com, ranj42@gmail.com, drlavanyakaparti@yahoo.com, drpradeep777@gmail.com
Abstract Background: Nonalcoholic fatty liver disease (NAFLD) is associated with severe abnormalities of the body including hepatic lipid metabolism. Lipid abnormalities such as fatty acid accumulation, ceramide overload and arachidonic acid metabolic disturbance are responsible for pathogenesis of NAFLD. NAFLD patients are at major risk of liver-related problems that leads to frequent liver transplantation. Liver biopsy is a gold standard for diagnosis of NAFLD but the other advancement in the techniques including non-invasive, genetic tests and biochemical analysis are providing futuristic approach for better understanding of the pathogenesis and targeted treatment. In this article, we have summarized the epidemiology, pathophysiology, risk factors, pathological changes, recent treatments and diagnosis techniques for the non-alcoholic fatty liver disease (NAFLD). This article defined the usefulness of ultrasonography for diagnosis of NAFLD. It is reliable, non-invasive and most accessible method for estimation of degree of steatosis. Further, understanding of lipid metabolism in NAFLD may help in the development of novel therapies. Keywords: NAFLD, hepatic steatosis, lipid, ultrasound, alcohol
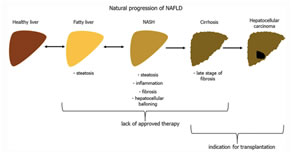
INTRODUCTION Non-alcoholic fatty liver disease (NAFLD) has become a big challenge to the medical science due to its complex pathogenesis, prevalence, lack of therapies and difficulties in diagnosis (Abd El-Kader and El-Den Ashmawy, 2015). The global prevalence of NAFLD is about 25%. It is predicted to become a leading cause of cirrhosis in the coming decade (Maurice and Manousou, 2018). NAFLD has become major cause of liver disease in children and adults that shows indication for liver transplantation. NAFLD is defined as micro- and macrovesicular steatosis having more than 5% hepatocytes (Table 1) (Carr et al., 2016). It is also associated with other disease manifestations like cardiovascular disease, hepatocellular carcinoma, liver fibrosis, sleep apnea and chronic kidney diseases (Fargion et al., 2014). All of these complications of NAFLD affects health, wealth and related burdens to the patients, their families and the society. NAFLD patients range from hepatic steatosis to non-alcoholic steatohepatitis (NASH). However, majority of the patients do not progress to NASH and other morbidities (Pei et al., 2020). The biopsy of liver is the current gold standard for diagnosis of the disease. Although, this diagnosis technique has certain limitations such as invasive nature, sampling variability and high cost (Papatheodoridi and Cholongitas, 2018). However, other non-invasive techniques have been also used such as imaging modalities for detection of steatosis, fibrosis and NASH. Interestingly, ultrasound is suggested as first-line screening tool for identification of steatosis in mass population (Zhang et al., 2018). Due to rapidly growing the cases of NAFLD, the efforts must continue for finding the accurate treatment and diagnostic techniques (Younossi, 2019). Ultrasonography of the liver is the most effective technique for the diagnosis of fatty liver in an individual (Mansour-Ghanaei et al., 2019). NAFLD is classified into three grades i.e. grade I, grade II and grade III that can be visualized on ultrasonography (Gao et al., 2013). Grade I is simple steatosis in which liver echogenicity is raised; Grade II is characterized by ballooning of liver and Grade III is characterized by ballooning of liver cells with fibrosis. In western population, NAFLD is a widespread etiologic agent responsible for development of chronic hepatic disease (Mustapic et al., 2018). However, it is rapidly growing in Asia-Pacific countries due to abruptly change in life style, food habits, increase use of fat containing stuffs, burden of diabetes mellitus and lack of exercise (Ashtari et al., 2015). The researches have been going on to determine the mechanism of diseases and possible treatment for this overload lipotoxic liver injury (Kozłowska-Petriczko et al., 2021). Thus, in this review we have discussed the epidemiology, and pathophysiology of NAFLD and incorporated recent advancements in the treatment therapies and management of the disease. The aim of this article was to define the diagnostic accuracy for detection of hepatic steatosis using ultrasound and other techniques. Figure 1 represents the schematic progression of NAFLD.
Figure 1: Schematic representation of progression of NAFLD
Table 1: Causes of hepatic steatosis
Epidemiology and other consequences of NAFLD NAFLD is characterized by deposition of excess macro vesicular fat more than 5% of the hepatocytes (Kneeman et al., 2012; Parthasarathy et al., 2020). NAFLD is prevalent in all countries of the world, however, in Western countries it affects about 20-30% of population in which 2-3% patients progress to hepatocarcinoma and liver cirrhosis (Bellentani et al., 2010). Males are more prone towards NAFLD than females, it increases with age and influences by lifestyle habits (Ballestri et al., 2017). The major limitation of NAFLD epidemiology is the non-availability of a disease-specific biomarker (Mitra et al., 2020). NASH and fibrosis are the other clinically relevant subsets of NAFLD that are histologically defined entities and therefore these are difficult to estimate in the epidemiological context (Peng et al., 2020). However, some non-invasive serum markers are used, in addition, imaging modalities for the assessment of disorders related to NAFLD. Unfortunately, serum markers lack uniformity, standardization and not accepted yet by wide community in epidemiological studies. Imaging modalities such as MRI can be used to measure liver fibrosis and fat with fair reproducibility but it is difficulty for large scale production due to limited availability, higher cost and lack of expertise in MRI (Li et al., 2018). Interestingly, ultrasound is the most acceptable equipment that is able to give epidemiological data on NAFLD and detect liver fat in a semi quantitative manner (Lupsor-Platon et al., 2021). In some studies, ALT has also used as a surrogate of liver injury but it is nonspecific in its simplicity and availability. Pathophysiology of NAFLD The pathogenesis of NAFLD is proposed to be a possible cause of fatty liver infiltration. The other clinical conditions such as steatosis, NASH and cirrhosis are suggested to be associated with the disease (Paschos and Paletas, 2009). It has proposed that metabolic syndrome plays a major role in the pathogenesis of NAFLD. The pathogenesis and detailed mechanism of NAFLD is an accumulation of fat with insulin resistance (Kitade et al., 2017; Utzschneider and Kahn, 2006). Additionally, activation of stellate cells and pro-inflammatory cytokines are the secondary cause of NAFLD (Stojsavljević et al., 2014). It has suggested by many researchers that reduction of body weight may stop development of NASH. The patients can be benefited by taking low sugar, increase fiber intake, regular exercise and healthy diet (Asif, 2014). Adipose tissue enlargement and metabolic complications are need to be investigated for critical etiopathogenesis of NAFLD. It has reported that Patatin-like phospholipase domain-containing protein 3 (PNPLA3) is responsible for remodeling of lipid droplets (Mitsche et al., 2018). PNPLA3 is a replicable and most robust genetic variant associated with NAFLD (Unalp-Arida and Ruhl, 2020). Other genetic variants such as glucokinase regulator and O-acyltransferase domain-containing 7 are involved in the regulation of insulin signaling, lipid metabolism, oxidative stress, inflammation and fibrogenesis and thus, responsible for progression of NAFLD. Figure 1 shows the pathophysiology of NAFLD. Figure 2: Schematic representation of progression of NAFLD Risk factors for NAFLD NAFLD is a disorder of hepatic steatosis that can be determined by histology or imaging. It is very all around the world in the form of chronic liver disease. The important risk factors for the development and progression of NAFLD are age, obesity, male gender, high cholesterol, sleep apnea, cardiometabolic alterations, hypo- and hyperthyroidism and insulin resistance. The complication of NAFLD includes ascites (fluid buildup in the abdomen), liver cancer, confusion, swelling of veins and hepatic encephalopathy (Duseja and Chalasani, 2013).
Diagnosis of NAFLD Diagnosis of NAFLD required history of patients for alcohol intake or any genetic disorders that may be responsible for phenotype of fatty liver. The suspicious patients are also evaluated for the level of triglycerides in the body, additionally, to check elevations of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) (Dumitrascu and Neuman, 2018). Table 2 shows diagnosis parameters for NAFLD suspicious patients. The person is diagnosed with computed tomography or ultrasound after abnormal liver function tests to scan liver for indications of fat infiltration. Diagnosis of NAFLD through ultrasonography requires specific instrumentation and expertise. Ultrasound technique is used by clinicians to identify attenuation of image, uniform heterogeneous liver, enlarged liver filling and thick subcutaneous depth. Ultrasound is an appealing imaging technique to identify hepatic steatosis due to ease of use, accessibility and low-side effect profile (Khov et al., 2014). However, ultrasound cannot replace liver biopsy to examine the degree of fibrosis.
Table 2: Evaluation of NAFLD suspicious patients
CONCLUSION It is expected that the health burden of NAFLD will rise in near future. It is due to aging population and less control over major disorders such as liver disease, alcoholic cirrhosis and hepatitis B and C. However, NAFLD is itself a risk factor for developing cardiovascular disorders and thus, results in increased liver-related mortality. The other components of metabolic syndrome such as diabetes, obesity and dyslipidemia should also be addressed. Modification lifestyle and losing weight remains the cornerstone of management of NAFLD. However, we are about to enter the new era having promising drugs for NAFLD and fibrosis.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. Home
Home