 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 2 - November 2017
A comparative study of serum sodium and potassium levels between pre-eclamptic patients and normal pregnant women
V Naga Guhan1, Sarita Basu2*, K Prabhakara Rao3, Mary Daniel4, S Arul Vijaya Vani5, S Priyadharshini6
{1Assistant Professor, Department of Biochemistry} {6Assistant Professor, Department of Anatomy} Al Azhar Medical College and Super Specialty Hospital, Thodupuzha, INDIA. 2Associate Professor, Department of Biochemistry, Meenakshi Medical College Hospital and Research Institute, Kanchipuram, INDIA. {3Professor and Head, Department of Biochemistry} {4Professor and Head, Department of Obstetrics and Gynaecology} Pondicherry Institute of Medical Sciences (PIMS), Pondicherry, INDIA. 5Assistant Professor, Department of Biochemistry, Mahatma Gandhi Medical College, Pondicherry, INDIA. Email: guhan.nagu@gmail.com
Abstract Background: Hypertensive disorders in pregnancy are one of the major causes of maternal and perinatal mortality and morbidity. Though various factors like placental ischemia, immunological maladaptations, genetics and susceptible endothelium have been shown to play etiological role, the exact pathogenesis and complications of preeclampsia still remains undivulged. Of late, electrolyte imbalance is gaining prominence in the aetiopathogenesis of preeclampsia. Aim: To estimate and compare the serum levels of electrolytes like sodium and potassium between preeclamptic patients and normal pregnant women Materials and Methods: This was a case control study done in Pondicherry Institute of Medical Sciences with 50 preeclamptic patients as cases and 50 gestationally age matched normal pregnant women as controls. After getting informed consent, serum sodium and potassium levels were measured from both cases and controls. Results: Serum potassium levels were significantly decreased (p < 0.001) in cases when compared to controls. Further hyponatremia (p- 0.003) and hypokalemia (p- 0.001) were strongly associated with preeclampsia. Conclusion: Hyponatremia and hypokalemia were more prevelant in preeclamptic women. Proper monitoring and appropriate correction of these parameters during early pregnancy can prevent hypertensive complications in pregnancy. Key Words: Potassium, preeclampsia, sodium
About 830 women die from pregnancy related complications around the world every day1.The major causes that account for 80% of all maternal deaths are severe bleeding, infections, hypertensive disorders followed by unsafe abortions. In developed countries like India, almost one fourth of maternal deaths are due to pre eclampsia and eclampsia.2 Preeclampsia is defined as high blood pressure (≥ 140/90 mmHg) and proteinuria(>300mg/day) after 20 weeks of pregnancy in a previously normotensive woman.3 Whereas eclampsia is defined as, seizures that cannot be attributed to other causes in a woman with pre-eclampsia.4 Though various theories have been proposed for the aetiopathogenesis of pregnancy induced hypertension, the most convincing among them is poor placentation. Inappropriate syncytiotrophoblast invasion and poor remodeling of uterine vessels leads to placental insufficiency. This triggers the complex mechanisms resulting in systemic endothelial dysfunction and the clinical syndrome of preeclampsia.5 Very recently, electrolyte imbalance is also gaining focus in the evolution of preeclampsia.6 The role of electrolytes like sodium and potassium in maintaining the normal vasculature and regulating the blood pressure is established by various researches7. So we measured the serum sodium and potassium levels in preeclamptic patients and compared with normal pregnant women to figure out their role in the pathogenesis and prevention of preeclampsia.
MATERIALS AND METHODS
Cases: Pregnancy Patients after 20 weeks of gestation with Controls: Gestational age matched normal pregnant women. Exclusion Criteria Patients with Renal diseases, Diabetes mellitus/Gestational DM, Chronic hypertension, Gestational hypertension(without proteinuria), Adrenal and other endocrine disorders and any other systemic illnesses. Blood samples were acquired from cases and controls after securing informed consent. After centrifuge, serum was separated and was assayed for sodium and potassium levels using electrolyte analyser which worked under the principle of potentiometry using ion selective electrode8. All data were expressed as mean ± SD. To compare the mean value of the parameters between cases and controls, ‘Student t Test’ was used whereas Chi square test was used to study the association between two variables. SPSS 17.0 software was used for all statistical analyses and ‘p’ value of ≤ 0.05 was considered as statistically significant.
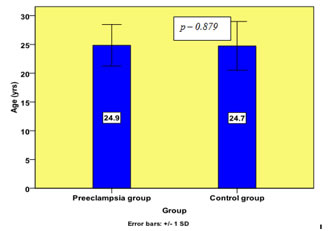
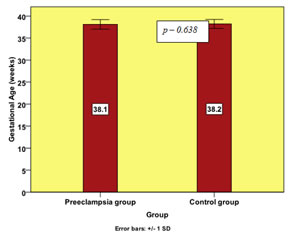
RESULTS In our current study, there was no significant difference in age and gestational age between cases and controls.
Figure 1: Comparison of age (yrs) of cases and control
Figure 2: Comparison of Gestational Age(weeks) of cases and controls
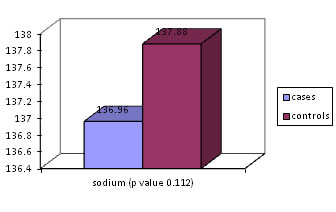
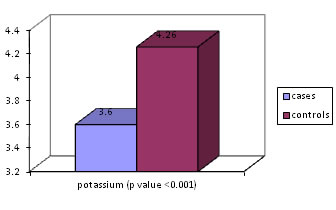
There was no significant difference in serum sodium levels between cases and controls whereas serum potassium levels falls significantly in preeclamptic women than compared to those in control group (Table 1).
Figure 3: Comparison of serum sodium(mmol/L) of cases and controls Figure 4: Comparison of serum potassium(mmol/L) of cases and controls Further serum sodium < 135 mmol/L (p value – 0.003) and serum potassium < 3.5mmol/L (p value – 0.001) were found to be strongly associated with preeclampsia.
Table 1: Association between hyponatremia and preeclampsia
Chi square test *; p value <0.05 – statistically significant
Table 1: Association between hypokalemia and preeclampsia
Chi square test *; p value <0.05 – statistically significant
DISCUSSION This research was carried out to compare the serum levels of sodium and potassium between gestational-age matched preeclampsia and normal pregnancy. In our study we observed that preeclampsia was found to be more common in primigravida (78% of preeclamptic women were primigravida). This contention is strongly supported by Kirsten Duckitt et al, who in their study, found that nulliparity triples the risk of preeclampsia.9 In preeclampsia group, 42 % of babies were born as low birth weight whereas in control group only 6% were low birth weights. We have a study by Xiong X et al, supporting the relation between preeclampsia and low birth weight, which states that women with preeclampsia were also at markedly higher risk of having low-birth-weight (adjusted odds ratio, 4.14; 95% confidence interval, 3.32-5.15)10 Serum sodium is postulated by various studies to play a trivial role in the pathogenesis of preeclampsia. There were contrasting reports stating that both hyponatremia and hypernatremia could be associated with preeclampsia. May N Yussif et al found that the serum sodium was significantly higher in preeclamptic women.11 Neeru Bhaskar et al found that dietary restriction of sodium could decrease the incidence of preeclampsia.12 But Indumathi V et al in their clinical trial proposed that decreased serum sodium lead to hypertension.13 Likewise, in our study too, hyponatremia (Na < 135 mmol/L) was found to be strongly associated with preeclampsia. There was a significant fall in serum potassium levels among cases in our study. Our findings are in accordance with those reported by other authors. Anjum K Sayyed et al in their clinical trial found that hypokalemia may have a key role in the pathogenesis of preeclampsia.14 Magna Manjareeka et al. found that the preeclamptic women of South India exhibit significantly lower serum potassium levels15 Extracellular sodium and potassium levels are maintained by the uninterrupted actions of Na+/K+ pump and Na+/K+ cotransporter across the cell membranes. Ulrich S et al, in his research work, accomplished that, in pre eclamptic patients, the net sodium extrusion by Na+/K+ cotransporter was abnormally low.16 This was further substantiated by a study done by Arumanayagam M et al.17 This could be the probable explanation for hyponatremia and hypokalemia encountered in our study among the preeclamptic women. Hyponatremia and hypokalemia increases the renin production and enhances the sensitivity of blood vessels to vasoconstrictors like angiotensin II and aldosterone. Further serum potassium mediates vasodilation through polarisation of vascular smooth muscle membrane. So any decline in serum sodium and potassium can cause vasoconstriction and hypertension.18
CONCLUSION Hyponatremia and hypokalemia documented in our study among the preeclamptic women has both diagnostic and therapeutic implications on the disease. In high risk population, estimation of these parameters in the early pregnancy can be done and its ability to predict the development of preeclampsia in the later pregnancy can be studied further. Proper monitoring and appropriate correction of these parameters during early pregnancy can be used as a preventive tool in preeclampsia.
REFERENCES
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.