 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 3 - December 2017
Ischemia modified albumin – A novel marker in diagnosis of myocardial ischemia
Junedi Mehraj A G1, Gaikwad S B2*
1Assistant Professor,2Professor and HOD, Department of Biochemistry, Government Medical College, Jalgaon-425001, Maharashtra, INDIA. Email: gaikwad62@rediffmail.com
Abstract Background: Early identification of patients with acute myocardial infarction is of prime importance due to the associated very high mortality. Only 30% of the patients presenting at emergency cardiology care with chest pain have coronary disease. A number of biochemical tests like CKMB and Troponin-T/I have been introduced for early detection of the coronary syndrome. Ischemia modified albumin (IMA) has been recently introduced as a marker of myocardial ischemia. Objective: To evaluate the diagnostic efficacy of ischemia modified albumin in patients admitted to the coronary care unit within 6 hours of chest pain. Materials and methods: Fifty healthy volunteers formed the control group from which the normal range was derived. IMA was significantly raised in ischemia patients than in controls. IMA demonstrated good discrimination between the ischemic and the non ischemic patients. Results: IMA showed a higher level in ischemic patients than in control with sensitivity 82% (P<0.001). IMA identifies 83.67% of acute myocardial infarction patients with high negative predictive value 82.35%. It detects the ischemia earliest before the necrosis of myocardium occurs, contrary to above other markers AST, Troponin I etc released from myocyte after necrosis of myocardium. Conclusion: IMA has evolved as cost effective, highly sensitive, early diagnostic marker of cardiac ischemia rather than necrosis and rule out test in AMI patients. Thus it allows beginning management of myocardial ischemic patients as earliest as possible. Keywords: Coronary artery disease (CAD), Ischemic modified albumin (IMA), Acute Myocardial infarction (AMI), Acute coronary syndrome (ACS), Cardiac Troponin (CTn).
Coronary artery disease (CAD) is predicted to be the leading cause of morbidity and mortality in developing countries by the year 20201,2. Approximately 30% patients presenting at emergency department with chest pain actually develop acute myocardial infarction (AMI)3. Myocardial ischemia results from the lack of adequate blood perfusion of the myocytes, leading to a deficiency of oxygen and nutrients, thus compromising their vital functions. The manifestations of the myocardial ischemia are varied and multiple like chest pain, epigastric or arm discomfort, breathlessness, nausea and vomiting. However, these symptoms may be subtle and are not easily recognized. Prolonged ischemia can lead to myocardial cell death known as acute myocardial infarction (AMI). Because of the varied presentation and associated high mortality, the early identification of patients with AMI is very critical for the patient management and has a bearing on the prognosis4. In a clinical setting, myocardial ischemia is assessed by an individual’s symptoms and electrocardiographic (ECG)5 studies. The ECG changes may include ST-T segment wave alterations5. Ideally, it is essential to identify myocardial ischemia before the onset of irreparable myocardial cell damage. Recently, a new parameter ischemia modified albumin (IMA) has been developed and observed to be very useful for the detection of acute myocardial ischemia that identifies the patients having potential coronary artery lesion, with high risk of adverse cardiac events. Unlike injury markers such as CK-MB, myoglobin, and troponin, IMA is believed to be a marker of cardiac ischemia. The IMA level rises within minutes after the onset of ischemia and remains elevated for several hours after the cessation of the ischemic event. IMA rises in the presence of ischemia and not as a result of necrosis6,7,8. IMA is produced when ischemia stresses released from hypoxic heart tissue induce modification of circulating albumin. IMA is defined as albumin modified by the free radicals produced in ischemic tissue9.
MATERIALS AND METHODS Fifty AMI patients between age group of 40-75 years admitted to the coronary care unit within 6 hours of chest pain were enrolled in the study during the period from May 2013 to September 2015. All of them were diagnosed on the basis of clinical examinations and ECG findings. Fifty age and sex matched healthy individuals without any history of coronary artery disease from the hospital staffs were taken as control. We measured following biochemical parameter Aspartate transaminase, Troponin I and Ischemic modified albumin (IMA). Albumin Cobalt Binding Assay (IMA): Principle: The assay is based on the premise that myocardial ischemia causes changes in human serum albumin (HSA) that are demonstrated by reduced exogenous cobalt (II) binding. The concentration of ischemia modified serum albumin can be determined by addition of a known amount of cobalt (II) to a serum specimen and measurement of the unbound cobalt (II) by colorimetric assay using dithiothreitol (DTT). An inverse relationship thus exists between the level of albumin bound cobalt and the intensity of the colour formation. Procedure: The whole process involved addition of 200(μl) of patient’s serum to 50 (μl) of COCl2 solution (1 g/L) followed by vigorous mixing and then 10 minutes of incubation. A volume of 50 (μl) of DTT (3 g/L) was then added and mixed well. After 2 minutes of incubation, 1 mL of 9 g/L solution of NaCl was added. The absorbance of the assay mixture was read at 470 nm wave length. The blank was prepared in the same way with the exclusion of DTT. I4
RESULTS Fifty patients admitted to ICCU of Shri Chatrapati Sarvopchar Rugnalaya and Civil Hospital, Solapur were selected for the study in the age group of 40 to 75 years. Among these subjects, 31 (62%) were male and 19 (38%) were female. Majority of the patients (74%) were between 46 to 75 years of age. The clinical data were noted down from the patient’s hospital files and correlated with laboratory data at the end of the study. Biochemical analysis of the study group revealed significant rise in total cholesterol in AMI patients as compared to controls. HDL-cholesterol and LDL-cholesterol also registered marked change in the AMI patients. The ischemic marker serum IMA documented a prominent rise in these cases, with a mean value of 215.5 U/micro L. The sensitivity for AST, troponin I and IMA in the diagnosis of MI are 60%, 80% and 83% respectively. The specificity for AST, troponin I and IMA in the diagnosis of MI are 70%, 80% and 84% respectively. The positive predictive value for AST, troponin I and IMA in the diagnosis of MI are 66%, 83% and 83.67% respectively. The negative predictive value for AST, troponin I and IMA in the diagnosis of MI are 63%, 80% and 82.35% respectively.
Table 2: Biochemical parameters in AMI patients and healthy controls (Mean+S.D)
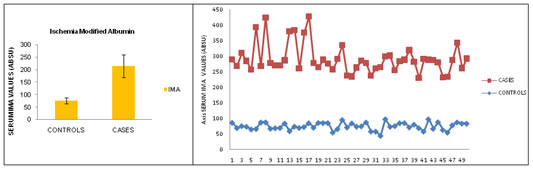
The levels of IMA in AMI and control subjects were depicted in Figure 1. The upper limit of the cut off value of serum IMA was taken to be 87 U/mL which was calculated from 95th percentile of 50 apparently healthy volunteers. This is close to the cut off value taken by Sbarouni et al12 and Sinha et al5 whereas it was taken to be 70 U/mL by Cui et al13. Figure 1 Figure 2 Legend Figure 1: Serum ima levels in (mean+s.d) in controls and cases; Figure 2: Distribution 0f serum ima values in controls and cases Table 2: Clinical performance of AST, Troponin I and IMA
DISCUSSION Atherosclerosis is one of the major causes of AMI10. Prolonged ischemia can lead to myocardial cell death and is a precondition to infarction11. Therefore, identification of myocardial ischemia at the earliest stage is very much essential to prevent the devastating consequences of the disease. Currently there is no well defined biochemical marker for identification of myocardial ischemia. Biochemical markers like CKMB, CTnT and myoglobin used in assessing cellular necrosis are not suitable for diagnosing myocardial ischemia12. From a diagnostic standpoint, the aim is to try to develop markers that can identify patients with AMI even when there is no evidence of myocytes Again in cases with cardiac ischemia, it may be more difficult to reach at a diagnosis when the patient has acute chest pain with a non diagnostic ECG and alteration in normal markers for necrosis. In such cases patients are at increased risk for subsequent coronary events but they may often be discharged because there is insufficient evidence to justify hospital admission6. Recently introduction of IMA assay that has received approval from the US Food and Drug Administration13 can be considered to be used to identify these ischemic patients as well as to rule out patients who do not have ACS. The present study registered a significant rise in serum IMA in AMI cases as compared to control, similar to the observations of the previous studies that distinguishes myocardial ischemic patients from non-ischemic patients14,15. Thus IMA appears to be a sensitive biomarker of myocardial ischemia in AMI patients presenting to the emergency department. Its ability to detect ischemia before myocytes destruction would allow for earlier and accurate management decisions as well as its role in a definitive biochemical ruling out strategy. While the specific molecular alterations and events that induce albumin modification have been only partially elucidated, better understanding of ischemic and reperfusion events at subcellular level needs further research in future.
ACKNOWLEDGEMENT Authors want to thanks Dr Hiroli, Assistant Professor from Department of Anatomy for his valuable support during Article Preparation.
CONCLUSION In transient myocrdial ischemia or injury from cardiac causes of chest pain is an important diagnostic trouble. In this emergency situation the clinicians, due to limitations are confuse in the diagnosis of chest pain. In this situation, IMA can be used to assess atherosclerosis-related myocardiac ischemia. It is also well understood that IMA increases within minites and remain elevated for several hours after the injury to cardiac muscles. IMA is an easy, non-invasive method to assess ischemia.IMA has evolved as cost effective, highly sensitive, early diagnostic marker of cardiac ischemia rather than necrosis and rule out test in AMI patients. Thus it allow to begins management of AMI earliest possible.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.