 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 2 - August 2018
Relation between uric acid and chronic kidney disease
Shakuntala Masti
Assistant Professor, Department of Biochemistry, S S Institute of Medical Sciences and Research Centre, Davangere -577004, Karnataka, INDIA. Email: shaku.jkd94@yahoo.com
Abstract Aims: To study the relationship of serum uric acid with chronic kidney disease and assess the relationship of increased serum uric acid as an established risk factor for chronic kidney disease. Materials and Methods: A hospital based study was conducted on 30 subjects with CKD were selected as cases and 30 subjects with normal kidney function tests were selected as controls for the present study. Results: Serum uric acid significantly increased (p<0.001) in cases compared to controls. Pearson’s correlation analysis showed a significant positive correlation between serum uric acid and serum creatinine(p<0.001) and negative correlation with eGFR(p<0.001). Conclusion: serum uric acid is significantly higher and strongly associated with chronic kidney disease. Key Word: serum Uric acid, serum Creatinine, eGFR and chronic kidney disease.
INTRODUCTION Chronic Kidney Disease(CKD) is now recognized as a common condition that elevates the risk of cardiovascular disease as well as kidney failure and other complications. The number of patients with kidney failure treated by dialysis and transplantation(the end stage of CKD) has increased dramatically in the United States from 209, 000 in 1991 to 472 ,000 in 2004. Earlier stages of CKD are defined based on the combination of kidney damage (most often quantified using albuminuria) and decreased kidney function (quantified as glomerular filtration rate [GFR] estimated from the serum creatinine concentration).1 A growing number of epidemiologic and experimental evidence suggests that uric acid is an independent risk factor for cardiovascular and renal disease.2,3 For patients with hypertension, heart failure or diabetes, hyperuricemia always predicts a high mortality. The mechanisms by which uric acid causes organ injury are still incompletely understood. However, increasing evidence suggests that uric acid is an agent of inflammation.4 Serum uric acid is commonly elevated in subjects with chronic kidney disease (CKD), but was historically viewed as an issue of limited interest. Recently, uric acid has been resurrected as a potential contributory risk factor in the development and progression of CKD. Pilot studies suggest that lowering plasma uric acid concentrations may slow the progression of renal disease in subjects with CKD.5 The objective of this study is to determine association of increased serum Uric acid in chronic kidney disease patients without Type 2 diabetes mellitus, which is one of the important risk factor for CKD.
MATERIAL AND METHODS The study subjects were selected based on inclusion and exclusion criteria a total number of 60 subjects, 30 subjects with CKD were selected as cases and 30 subjects with normal kidney function tests were selected as controls for the present study. A proforma was used to record relevant information and study subjects.
-Kidney damage for more than 3 month -GFR <60ml/min/1.73m2 Exclusion criteria
Controls: 30 age and sex matched healthy controls in the age group of 40 -80 years. Collection of blood samples for the study 3ml of venous blood is collected under aseptic precaution in a sterile bulb from selected subjects. Then the serum is separated by centrifugation which is used for estimation of uric acid and creatinine. In all the subjects, concentration of serum uric acid6 (enzymatic uricase method) and serum creatinine7 ( Modified kinetic Jaffe’s method) estimated by semi-auto analyser and eGFR is calculated by Modification of Diet in Renal Disease (MDRD) formula1 eGFR (ml/min/1.73 m2) = 186 × serum creatinine(mg/dl)1.154× (age)-0.203× 0.742 (if female).
RESULTS A total of 30 cases and 30 controls were taken for this study.
Table 1:Showed 18 males and 12 females with CKD cases and age distribution among controls and cases are 47±6yrs and 55 ±8yrs.
Table 2: Mean concentrations of serum Uric acid, Creatinine and eGFR:
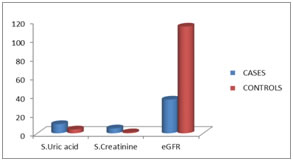
Table b showed the mean concentrations of serum levels of uric acid in controls and cases are 4.1±1.4mg/dl and 9.8±1.2mg/dl, which indicates Serum uric acid significantly increased (p<0.001) in cases compared to controls. Mean concentrations of serum creatinine levels in controls and cases 1.05±0.35 mg/dl and 5.2±1.4 mg/dl and mean concentrations of eGFR controls and cases 114±5.65 ml/min/1.73m² and 36.5±12.02 ml/min/1.73m²
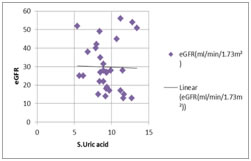
Graph 1: Comparison of serum Serum uric acid, Serum Creatinine(mg/dl) and eGFR(ml/min/1.73m²) Levels among study group Graph 2: Relation between serum Uric acid and eGFR: The statistical analysis by unpaired student’s t-test showed that mean concentration of serum level of Serum uric acid significantly increased (p<0.001) in cases compared to controls. Pearson’s correlation analysis showed a significant positive correlation between serum uric acid and serum creatinine(p<0.001)and negative correlation with eGFR(p<0.001).(Table b, graph a, graph b)
DISCUSSION Chronic kidney disease (CKD) has become a public health challenge and is a common disorder . For example, about 20% of adults have CKD, which is defined as kidney damage or a glomerular filtration rate (GFR) <60 ml/min/1.73 m2 for at least three months regardless of cause8 Several but not all prospective studies have suggested a significant association of hyperuricemia with the development and progression of kidney disease in mainly nondiabetic populations.Giacomo Zoppini et al found that elevated uric acid levels were associated with an increased risk of incident CKD, independently of a broad spectrum of established risk factors, including hypertension, diabetes-related variables, and renal function measures. Thus, it is conceivable that hyperuricemia might confer an excess risk over and above the risk attributable to underlying established risk factors.9 Recently, uric acid has been resurrected as a potential contributory risk factor in the development and progression of CKD. Most studies documented that an elevated serum uric acid level independently predicts the development of CKD.5 In animal models, elevated uric acid levels can lead to arteriolopathy of preglomerular vessels, impaired autoregulation, glomerular hypertension, as well as endothelial dysfunction.10 In our present study mean concentration of serum uric acid levels increased (9.8±1.2mg/dl) in CKD cases compared to controls(4.1±1.4mg/dl ) as it goes with the same findings Giacomo Zoppini et al without established risk factor like diabetes mellitus for CKD. Rudolf P. Obermayr et al study found that diuretics are associated with an increase in serum UA levels, and it is suggested that raising UA levels can stimulate the renin-angiotensin-system accelerating the development of renal microvascular disease and thereby predispose the patient to renal disease progression. Thereupon, in humans, asymptomatic hyperuricemia induced progression of CKD . hyperuricemia may be one of the key mechanisms for the activation of the renin-angiotensin and cyclooxygenase-2 systems in progressive renal disease, which could be mediated by its effect to upregulate angiotensin-1 receptors on vascular smooth muscle cells.11 In our study increased serum uric acid levels associated with the decreased eGFR which indicates decrease in renal function, these findings are in accordance with study Dong-Hyuk Jung et al showed that an increase in uric acid of 1 mg/dL is independently associated with a GFR decrease of about 5 mL/min/1.73 m2 in men and about 6 mL/min/1.73 m2 in women.12 Duk-Hee Kang et al investigated that uric acid may induce renal disease via an induction of afferent arteriopathy as a consequence of an altered proliferation and senescence of vascular cells, an induction of local oxidative stress and inflammation with an activation of RAS, followed by impaired peritubular capillary circulation and renal ischemia. Uric acid-induced phenotypic transition of renal tubular cells also could be important13 Richard J. Johnson et al showed that an elevated uric acid has been reported to predict the development of renal insufficiency in individuals with normal renal function. Uric acid is an independent predictor for progression in IgA nephropathy. Hyperuricemia also correlates with the development of renal dysfunction in type II diabetes100 and independently predicts progression in renal transplant patients on.14 In our study we have excluded CKD with diabetes mellitus which is one of the established risk factor for CKD.Our findings are in accordance with the studies like Loretta Cain et al and Masatoshi Kawashima1 et al. Loretta Cain et al examined the association between serum uric acid and CKD among study subjects free of diabetes and hypertension, the results were found to be consistent with the main multivariable findings, suggesting an association independent of diabetes and hypertension.15 Our study has selected CKD cases and controls age group between 40-80 yrs, this in accordance with the study like Masatoshi Kawashima1 et al, which investigated the associations between new-onset CKD and asymptomatic hyperuricemia without gouty attacks, low serum HDL-C, hypertension, diabetes and obesity in Japanese male factory workers over 40 years of age. The results showed a significantly higher incidence of new-onset CKD in participants with asymptomatic hyperuricemia. In this study, the hazard ratio for asymptomatic hyperuricemia was greater than those for other factors, including hypertension16
CONCLUSION As a conclusion, serum uric acid levels are significantly higher and strongly associated with Chronic kidney disease without established risk factor like diabetes mellitus. This indicates increased uric acid levels in blood may have role in progression of Chronic kidney disease. Hypouricemic drugs can be used to control the progression of the CKD.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.