 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 3 - September 2018
Association of serum calcium level with metabolic syndrome: A case-control study
Sagar Dholariya1, Prashant K Nichat1*, Leela G Abichandani2
1Assistant Professor, Department of Biochemistry, R. D. Gardi Medical College, Ujjain-456006, Madhya Pradesh, INDIA. 2Professor, Department of Biochemistry, Grant Government Medical College, Mumbai, Maharashtra, INDIA.
Abstract Background: Metabolic Syndrome (MetS) is highly prevalent in urban India. Circulating calcium has direct association with vascular disease like cardiovascular disease Calcium play crucial role in proper function of the insulin and lipid metabolism. Objectives: To assess serum calcium level in MetS patients and it association with parameters of the MetS Materials and Methods: It was a hospital based case control study. A total of 50 MetS cases and 50 age-matched healthy controls were included in the study. Cases were selected according to revised IDF criteria for MetS. Estimation of serum calcium, fasting blood sugar, triglyceride and HDL were done on advia 1800 chemistry autoanalyzer. Results: Serum calcium was found higher in MetS patients compared to controls. Mean ± SD value of serum calcium among cases and controls were 10.1 ±0.85 and 9.3 ± 0.62 mg/dl respectively (P<0.0001).We found significant association of calcium with FBS and serum triglyceride level with calcium. Both FBS (P=0.01) and triglyceride level (P=0.02) increased linearly with increases in calcium. There was no significant association of waist circumference, serum HDL and blood pressure with serum calcium level. Conclusion: Serum calcium level was high in metabolic syndrome cases compared to controls. Serum calcium has significant association with fasting blood sugar and triglyceride level. Key Words: serum calcium level, metabolic syndrome.
Metabolic Syndrome (MetS) is highly prevalent in urban India.1 Sedentary life style and overweight are important risk factors for development of MetS.2 MetS are characterized by presence of central obesity, insulin resistance, hypertension, glucose intolerance and dyslipidemia.3 MetS itself contain multiple metabolic risk factor that increase mortality. It increase the risk of development diabetes mellitus 2 by fivefold and cardio vascular disease by 2 fold.4 Calcium is most important intracellular messenger that regulate various biological function of the body.5 Calcium homeostasis is regulated in body by dietary intake, vitamin D and parathyroid hormone.6 Calcium play crucial role in proper function of the insulin7 and lipid metabolism.8 Altered calcium level has been associated with decreased insulin sensitivity and diabetes mellitus type 2 development.9 This decrease in insulin sensitivity has been due to decrease in number glucose transporter, GLTU4 in adipocyte.10 Intracellular calcium also play important role in cardiovascular function by regulating blood pressure. High intracellular calcium cause more influx of calcium in vascular smooth muscle cells that lead to increase peripheral resistance and development of hypertension. But dietary calcium supplement has been associated with decrease in blood pressure due to suppression of parathyroid hormone.11Association of calcium with metabolic syndrome and its components has been reported in various studies but its results are inconclusive.12, 13 Based on above knowledge, aims of our study to assess serum calcium level in MetS patients and it association with parameters of the MetS MATERIAL AND METHODS It was a hospital based case control study. The study was conducted in department of Biochemistry and Medicine at grant medical college. The study was approved by ethical committee of grant medical college. Patients attending medicine OPD with central obesity were main target of our study. Fifty MetS cases and fifty age and sex matched healthy controls were included in the study. Detailed history and informed consent were taken from all participants. Inclusion Criteria: Cases were selected according to revised IDF criteria14 for MetS as described below: Presence of central obesity and any two of the following factors like increase FBS level (≥ 100 mg/dl), increased triglyceride level (≥ 150 mg/dl), increased blood pressure (systolic BP ≥ 130 or diastolic BP ≥ 85 mm Hg) and decreased HDL level (< 40 mg/dl in males, <50 mg/dl in females). Cases of both sex and age between 30-65 years were included in the study. Exclusion Criteria: History of hypothyroidism or on its treatment, alcoholics, patient with human immune deficiency virus infection, liver diseases, pregnant women, hyperparathyroidism or hyperparathyroidism, kidney disease were excluded from the study. Patients were on calcium and vitamin D supplements were also excluded from the study. Waist circumference was measured by measuring tape at the level of anterior superior iliac spine. Mercury sphygmomanometer was used to measure blood pressure. Blood pressure was measured in sitting position with properly supported arm. Sample Collection: Five ml blood was collected form peripheral vein by venepuncture in morning after 12 hours of fasting. Blood was transferred in pain vial and fluoride vial. Serum was separated from plain vial after centrifuge it 3000 rpm for 15 minutes. Serum was used to assess serum calcium and lipid profile. Blood in fluoride vial was used to assess blood sugar level. Estimation of serum calcium, fasting blood sugar, triglyceride and HDL were done on advia 1800 chemistry autoanalyzer. Biological reference range of calcium was 9.3 – 11.0 mg/dl. Statistical Analysis: Statistical analysis was done by using SPSS version 16. The graphs and tables were done on ms excel 2010. Qualitative variables were analyzed by Pearson’s chi-squared test and Fisher's exact test. Unpaired-t-test and one way ANOVA were used for qualitative variables. P value <0.05 was considered as a statistical significant. The study was conducted on total 100 subjects. Percentage of male and female were 45.23 % and 53.44 % respectively. There was no significant difference of gender and religion among cases and controls. There was no significant difference of age among cases and controls (P>0.005). We found significant differences of waist circumference, FBS, serum triglyceride level, serum HDL level and blood pressure among the cases and controls (P<0.001) (Table 1).
Table 1: Baseline characteristic and MetS parameter in cases and controls
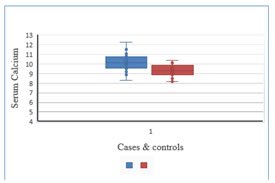
*Unpaired-t-test Mean ± SD value of serum calcium among cases and controls were 10.1 ±0.85 and 9.3 ± 0.62 mg/dl respectively. Serum calcium was found higher in MetS patients compared to controls. The difference of calcium among cases and controls was significant (P<0.0001) (Table 2).
Table 2: Serum calcium level in cases and controls
*Unpaired-t-test Figure 1: Box plot showing calcium level in cases and controls
Table 3: Association of serum calcium level with MetS parameters
*One-way analysis of variance for continuous variables
To know the association of serum calcium level with MetS parameters, cases were divided into three groups like < 9.5 mg/dl, 9.5-10.5 mg/dl and >10.5 mg/dl. We found significant association of calcium with FBS and serum triglyceride level with calcium. Both FBS (P=0.01) and triglyceride level (P=0.02) increased linearly with increases in calcium. There was no significant association of waist circumference, serum HDL and blood pressure with serum calcium level.
DISCUSSION Metabolic syndrome is emerging problem in India and increased risk of cardiovascular disease.15Circulating calcium has direct association with vascular disease like cardiovascular disease.16We hypothesize that calcium may be a risk factor for development of cardiovascular risk factor in MetS. We conducted population based cross sectional study to assess serum calcium level in MetS patients and it association with parameter of MetS. We found that calcium level was more in MetS patients compared to controls group. Results obtained by SaltevoJ, et al. (2011),17 and Park SH et al (2012)18 were support our results. High calcium level in MetS could be due to increased absorption of calcium from intestine and kidney and increased bone resorption.17It has been reported that higher PTH hormone were found in MetS and it is independent risk factor for development of MetS. High calcium in MetS could be due to increased PTH.19 We found linearly increased in calcium was associated with linearly increased in fasting blood sugar and triglyceride level. There was significant association of serum calcium level with fasting blood sugar and triglyceride level. Cho GJ (2012)20 was also found calcium association of FBS and triglyceride in MetS. Association of calcium and triglyceride could be due to decreased cholesterol metabolism by calcium.21Calcium cause decrease insulin sensitivity by decreasing number of GLUT4 transporter in adipocyte and it cause significant association between calcium and FBS.10High calcium level in MetS could be a reason for deranged lipid profile, insulin resistance and risk for developing cardiovascular disease. Limitations: Study should be done on larger population with vitamin D, PTH and insulin assessment to validate the results of study
CONCLUSION Serum calcium level was high in metabolic syndrome cases compared to controls. Serum calcium has significant association with fasting blood sugar and triglyceride level.
REFERENCES
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.