 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 3 - September 2018
Decreased serum adiponectin is associated with carotid atherosclerotic changes in type 2 diabetes mellitus patients
V Hariharan1, S Ramya2*, V C Renju3, S Sethupathy4
1Assistant Professor, Department of Biochemistry, Karpagam Faculty of Medical Sciences and Research, Coimbatore, Tamil Nadu, INDIA. 2Assistant Professor, Department of Biochemistry, Sree Annapoorna Medical College, Salem, INDIA. 3PhD, Department of Biochemistry, Sree Mookambika Institute of Dental Sciences, Kanyakumari, Tamil Nadu, INDIA. 4Professor and HOD, Department of Biochemistry, Rajah Muthiah Medical College, Annamalai Nagar, Tamil Nadu, INDIA. Email: drhariharanv@gmail.com
Abstract Background: Cardiovascular disease is the leading cause of death in world. The early detection of cardiovascular disease and risk identification is paramount to prevent and treat this condition. Even though many risk predictors like lipid profile, early Electrocardiogram changes exist, we need a marker which can predict the occurrence of the cardiovascular events more earlier. Serum Adiponectin is emerging as a risk predictor and a novel biomarker for Coronary vascular disease. Aims: In this study, we investigated the relationship of serum adiponectin levels and carotid intima media thickness in type II diabetic individuals. Materials and Methods: 48 known type II diabetics (aged 35-55 yrs) attending Diabetic OPD on treatment with oral hypoglycemic drugs were taken as study subjects. Anthropometric and metabolic assessments including serum Adiponectin levels were done. B-mode ultrasound imaging of the both common carotid arteries was used to measure common CIMT (Carotid intima-media thickness). Results: CIMT were higher in subjects with hypoadiponectinemia (p<0.013) than subjects with normal adiponectin levels. Serum Adiponectin was negatively associated with age (P<0.05), Conclusion: In diabetic patients, decreased serum adiponectin levels may lead to atherosclerosis of blood vessels and measurement of this can be a good predictor of future vascular events. Key Words: Adiponectin. Carotid intima media thickness. Carotid atherosclerosis. Type 2 diabetes.
Cardiovascular disease (CVD) is the leading cause of mortality in patients with type 2 diabetes and identification of individual risk patterns is fundamental for the prevention and treatment of CVD1. Adiponectin is a 30-kDa adipocyte-derived vasoactive peptide and it was found to be decreased in obesity2. Hypoadiponectinemia is associated with insulin resistance3, type 2 diabetes4, dyslipidemia5, and hypertension6. It has anti-inflammatory and antiatherosclerotic properties on endothelial cells by decreasing vascular inflammation, foam cell formation, and cell adhesion, which all are involved in the initiation and progression of vascular lesions2. Low levels of adiponectin have been associated with hypertension7, impaired endothelium dependent vasodilation8, increased risk of myocardial infarction in men regardless of the presence of diabetes9,10 and ischemic cerebrovascular disease11 Carotid intima-media thickness is a measure of subclinical atherosclerosis and is predictive of future myocardial infarction and stroke12-15. Carotid IMT was significantly greater and the levels of adiponectin were significantly lower in individuals with insulin resistance than those in normal subjects16. We therefore examined that whether circulating adiponectin levels are reduced in Type 2 diabetes, which may lead to sub clinical atherosclerosis and subsequent vascular events which can be detected by measuring carotid IMT.
MATERIALS AND METHODS Subjects: The study was approved by the Medical Ethics Committee of the institution, and all participants provided written informed consent. 48 (males =16, females=32) known Type 2 diabetic patients aged 35-55 yrs on oral hypoglycemic drugs were recruited in diabetic out-patient department of Rajah Muthiah Medical College Hospital, Chidambaram. Medical history did not reveal recent illnesses and physical examination did not show pulmonary or cardiac abnormalities. Known cardiovascular disease, renal function abnormalities, patients using insulin were exclusion criteria, but the use of antihypertensive medication was allowed. Body mass index (BMI) was calculated as weight divided by height squared (kg/m2). Systolic and diastolic blood pressure was measured after 15 min rest with a sphygmomanometer in sitting position. Anthropometric measurements were done. Blood samples were collected and ECG taken. Biochemical indices: Serum samples were taken after an overnight fast in clot activator tubes and centrifuged immediately and stored at -200C. Fasting plasma glucose was done by GOD-POD (Glucose Oxidase-Peroxidase) method, Total cholesterol (CHOD-PAP), HDL and LDL by Direct methods, insulin assay by RIA (Radio immuno assay), Liver function tests and Renal fuction tests were done. Serum adiponectin measured by Direct ELISA using kit from Thermofisher Scientific Co. Homeostasis model assessment was taken as a measure of insulin sensitivity (homeostasis model assessment; HOMA ir) using the equation: (fasting plasma insulin x glucose)/40517. Carotid Doppler: A B-mode ultrasonogram was used to view carotid arteries. An experienced Radiologist did the study for all the patients. Bilateral common carotid arteries were visualized with the patients lying in supine position and the greatest intima-media thickness was noted. Focal atherosclerotic plaque was defined as a clearly identified area of focal increased thickness (≥ 1 mm) of the intima-media layer. In the presence of plaque in the examined carotid segments, the maximal plaque length and the maximal plaque thickness and percentage of stenosis were also measured. Measurements on both sides were averaged to obtain the mean IMT, which defines the carotid IMT of each patient in this study. Statistical Analysis: Distributions of baseline characteristics were described using mean (S.D.) or median as appropriate. All P values < 0.05 were interpreted as statistically significant. All calculations were performed using a standard statistical package (SPSS 13.0, SPSS Inc., Chicago, IL, USA). Independent t test and pearson correlation analysis were done using the software.
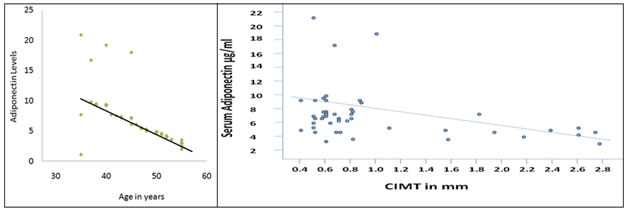
RESULTS Characteristics of study subjects: 48 patients (mean age=46.5yrs) were taken for the study and their BMI (mean=24) calculated and systolic(mean=124mmHg) and Diastolic blood pressure (mean=78.3mmHg) recorded. Mean Fasting blood glucose was 143.7 mg/dL. Only 9 Patients showed abnormal lipid profile. ECG showed perfusion abnormalities in 9 patients. One patient showed increased serum Alkaline phosphatase level. No major abnormalities of Serum electrolytes were observed in any of the subjects. 4 patients had moderately increased levels of uric acid. Serum Adiponectin levels seemed decreased with age (p<0.05) (Fig. 1). The study subjects were divided into two groups according to Serum Adiponectin levels. Group 1 (n=32) are the patients with normal adiponectin levels adjusted for age and gender and group 2 (n=16) were taken as subjects having low Adiponectin levels adjusted to gender and age. The general tests values of both groups are given in Table 1. No significance between any parameter based on adiponectin levels observed between two groups. CIMT levels significantly increased (p<0.013) with decrease in Adiponectin levels (Table 2). This relation is graphically expressed in Fig. 2. Carotid intima media thickness: Calculated mean IMT of both right and left common carotid arteries of all patients is 1.08mm. In the first group of 36 patients having normal adiponectin levels the mean IMT is 0.72mm.The second group of 12 patients having low adiponectin had mean IMT of 1.44mm (Table 2).
Table 1: Comparison of between cases and controls
Table 2: Comparison of Carotid IMT between both groups
Figure 1 Figure 2 Figure 1: Relation between age and serum Adiponectin values; Figure 2: Correlation between carotid intima-media thickness (IMT) and total adiponetin. The carotid IMT is significantly negatively associated with adiponectin (P < 0.05) DISCUSSION The adipose tissue secretes a broad range of hormone-like molecules called adipokines, which are involved in obesity related metabolic abnormalities and chronic inflammation. Their low plasma concentrations are associated with obesity, insulin resistance, and cardiovascular disease18. Adiponectin is an exceptional adipokine because it seems to be protective against atherosclerosis, and the determination of plasma levels may help to assess the risk of coronary artery disease. A vasoprotective effect of adiponectin is supported by in vitro studies showing that adiponectin decreases the expression of adhesion molecules on endothelial cells19, Suppresses foam cell formation by macrophages20, and inhibits vascular smooth muscle migration21. In this study we observed that in Type 2 Diabetes patients, Carotid IMT were higher in subjects with lower adiponectin levels. Subjects with normal or higher adiponectin levels had normal IMT. Our study is consistent with the findings observed by Horakawa et al, that low total Adiponectin levels in Diabetic patients had higher cardiovascular risk22. Diabetes Mellitus Per se can cause dyslipidemia leading to altered adipose tissue metabolism leading to reduced production of adipokines23. This reduction in adiponectin may lead to atherosclerosis which is a predisposing factors of vascular events. In future, Adiponectin can serve as a marker for subclinical atherosclerosis and can be used to predict future vascular events. Since Adiponectin exerts its effect by increasing HDL levels and decreasing LDL levels24,25,26, it is not clear whether Adiponectin is a better predictor than lipid profile in predicting CVD. We did not find any association between fasting plasma glucose, lipid profile, liver and renal function tests toward serum adiponectin levels or Carotid IMT. Previous studies had demonstrated the relationship between Insulin resistance and adiponectin17, but we did not find correlation between them. We found a relationship between age of the subjects and serum adiponectin levels. We found that adiponectin decreases with age (p<0.05). This is a new finding and it confirms the already proved theory that older individuals are more prone for atherosclerosis and vascular events. Previous studies27,28,29 has noted a positive correlation between age and carotid IMT, but we did not observe the same.
CONCLUSION In conclusion, our findings indicate a negative relationship between serum adiponectin and Carotid IMT. This proves that Serum adiponectin can be used as a marker for atherosclerosis in type 2 Diabetes for early intervention and prevention of full blown cardiovascular and cerebrovascular events. Limitation of this study: We performed this study in only a small number of subjects. A large sample study is needed to demonstrate clearly the relationship between Carotid IMT and serum adiponectin levels in diabetic individuals.
REFERENCES
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.