 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 8 Issue 2 - November 2018
A study of serum homocystein level and it’s association with lipid profile at a tertiary health care centre
Mohammad Rafi1, M Vijay Mohan2*
1Professor & HOD, 2Professor, Department of Biochemistry, RVM Institute of Medical Sciences & Research Centre, Laxmakkapally(V), Mulugu(Mdl), Siddipet District, Telangana, INDIA. Email: warangalmetro@gmail.com
Abstract Background: Coronary artery disease (CAD) is one of leading cause of death among the Indians. Hyperhomocysteinemia has been strongly linked to CAD. Lipid profile among the CAD patients shows elevated sr. cholesterol and serum triglycerides. This study was conducted to find any association between lipid profile and serum homocysteine level. Aim and objective: To study the association of lipid profile with homocystin level in patients of coronary artery disease. Methodology: Total 60 patients were studied. Group A participants were CAD patients and Group B were controls. Data was collected with pretested questionnaire. Srhomocysteine and lipid profile form both the groups were collected. Data was analyzed to see association in lipid profile and serum homocysteine level in the patients. Result: Serum Homocysteine level in CAD patients was 21.6±5.42 μmol/L and in control group it was significantly less (11.2±3.5 μmol/L).Serum cholesterol level in hyperhomocysteinemia group(178.6±36.6 μmol/L) was significantly more than the group with lower sr. homocysteine(153.2±21.4 μmol/L) Serum LDL level in group with higher homocysteine (105.21±23.2 μmol/L) was significantly more than the other group (28.43±9.6 μmol/L). Key Word:
INTRODUCTION Coronary artery disease is a major noncommunicable disease in India. It’s prevalence is increasing over period. As the age increases, coronary arteries that supply the heart with oxygen and nutrients develop atherosclerotic plaques in their walls. It has various risk factors like smoking, diabetes mellitus, obesity, hypertension, stress and physical inactivity. Cardiovascular disease (CVD) is considered as the first leading cause of death in the world. More people die annually from CVDs than from any other cause1. Homocysteine is a nonessentialsulphur containing amino acid that is obtained from metabolic demethylation of essential amino acid methionine. Several homocysteine species have been identified in human plasma including albumin-(protein)-bound, free circulating disulfides and sulfhydryl forms2. In previous studies homocysteine (Hcy) was established as a risk factor in coronary artery diseases.3,4,5 Hyperhomocystinemia can occur due to genetic or nutritional deficiency of folate, vitamin B12 or vitamin B6. Coronary artery disease was associated with increased levels of cholesterol. Both the lipids and homocysteine levels were high in the coronary artery disease. Studies were limited and restricted only to report the traditional risk factors including lipid abnormalities and serum homocysteine level and their association with CAD. Present study was conducted to find the association of lipid profile and serum homocysteine level in coronary artery disease patients.
MATERIAL AND METHODS Present study was a comparative study carried out in a tertiary care center in department of Biochemistry. Study population was patients with coronary artery disease and healthy patients. Inclusion criteria: 1. Patients clinically diagnosed as coronary artery disease. 2. Patients above age of 18 years and below 60 years. Exclusion criteria: 1. Patients below 18 years and above 60 years. 2. Patients not willing to participate. 3. Patients with history of diabetes milletus, renal disease and thyroid disorders. After inclusion and exclusion criteria total 60 patients were studied during a period of 6 months who were diagnosed as case of coronary artery disease. Group A consists of 30 patients with coronary artery disease and Group B contains 30 normal healthy individuals who were controls. Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining the study to them. Data was collected using pretested questionnaire. Data collection included sociodemographic profile of the patients. Detailed history and detailed clinical examination was done. fasting blood samples of about 8ml were drawn; serum was separated and analysed for Total cholesterol (TC), Triglycerides (TGL)and Automated High density lipoprotein (A-HDL) cholesterol using the Siemens Dimension auto analyser. The plasma was used for the estimation of Hcy by HPL CFluorescence detection with internal standard method6,7. According to the The American Heart Association total homocysteine plasma concentrations is classified as 5-15 μmol/L homocysteine as normal, 16-30 μmol/L homocysteine as moderate, 31-100 μmol/L homocysteine as 19 intermediately elevated and total homocysteine levels above 100 μmol/L as severely elevated concentrations8. Data was analysed using appropriate statistical tests to see the association of lipid profile and serum homocystein level.
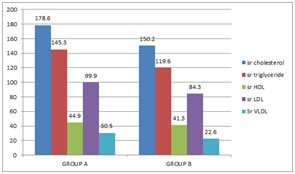
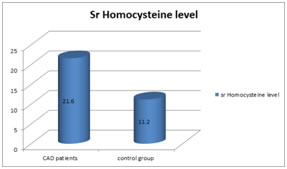
RESULTS Total 60 patients were studied. Group A had 30 patients who were diagnosed as CAD patients and Group B had 30 controls. Mean age of the patient was 37.7± 8.56 years. Mean age of Group A was 35.6± 5.73 years and of Group B was 34.21 ±4.3 years. Majority of the patients were male 36(60%). Female constituted 40% of all patients. In present study mean serum total cholesterol in CAD patients was 178.6±35.6 mg/dl whereas in control group it was 150.2± 27.3 mg/dl. Significant difference was observed in both the groups. It was observed that mean serum triglyceride in CAD patients was 145.3±11.9 mg/dl whereas in control group it was 119.6± 21.3 mg/dl. The mean serum HDL in CAD patients was 44.9±9.2 mg/dl whereas in control group it was 41.3± 8.4 mg/dl. Mean Serum LDL in CAD patients (99.9±25.6mg/dl) was significantly more than that of control group (84.3±11.2 mg/dl). Serum VLDL in both the group was comparable but it was more in CAD patients (30.5±9.5mg/dl) as compared to control group(22.6±7.6mg/dl). Figure 2 shows serum homocysteine level in CAD patients and control group. Serum Homocysteine level in CAD patients was 21.6±5.42 μmol/L and in control group it was significantly less (11.2±3.5 μmol/L). Table 1 shows distribution of patients according to serum homocysteine level and lipid profile. We analysed the data according to serum homocysteinelevel. if serum homocysteine was > 15 μmol/L it was considered as hyperhomocysteinemia. Serum cholesterol level in hyperhomocysteinemiagroup(178.6±36.6 μmol/L) was significantly more than the group with lower sr. homocysteine(153.2±21.4 μmol/L) Serum triglyceride level in hyperhomocysteinemia group was 152.1± 25.4μmol/L whereas in the group with lower sr. homocysteine it was 140.7± 26.8μmol/L. serum HDL level in both the groups is comparable. Serum LDL level in group with higher homocysteine (105.21±23.2 μmol/L) was significantly more than the other group (28.43±9.6 μmol/L). serum VLDL in both the groups was comparable. Figure 1: comparison of lipid profile in coronary artery disease patients and control group
Figure 2: comparison of serum homocysteine level in CAD patients and Control group
Table 1: Distribution of patients according to srHomocysteine level and lipid profile
DISCUSSION Total 60 patients were studied. Group A had 30 patients who were diagnosed as CAD patients and Group B had 30 controls. In present study mean serum total cholesterol in CAD patients was 178.6±35.6 mg/dl whereas in control group it was 150.2± 27.3 mg/dl. Significant difference was observed in both the groups. Mean serum triglyceride in CAD patients was 145.3±11.9 mg/dl whereas in control group it was 119.6± 21.3 mg/dl. Mean Serum LDL in CAD patients (99.9±25.6mg/dl) was significantly more than that of control group (84.3±11.2 mg/dl). Serum VLDL and serum HDL in both the group was comparable. Similar findings were observed in Chambers J.C. et al9. In our study Serum Homocysteine level was 21.6±5.42 μmol/L and in control group it was significantly less (11.2±3.5 μmol/L).in accordance with our study Shenoy V et al 10also observed higher level of srhomocysteine in patients. Increased plasma Homocysteine leads to the formation of atheromatous changes, which ultimately cause MI. Homocysteine contains reactive sulfhydryl group, which undergoes oxidation to the disulfide at physiological pH. The reaction is catalysed by transition metals and a variety of reactive oxygen species are produced which initiate lipid peroxidation responsible for endothelial cytotoxicity Most studies state that an elevated Homocysteine can increase the oxidative stress and inflammation of the vascular endothelial cells and thereby decrease the production of nitric oxide which is a strong relaxing factor .Homocysteine also increases HMG CoA reductase which increases cholesterol synthesis and hence atherosclerosis.10 Serum cholesterol level in hyperhomocysteinemiagroup (178.6±36.6 μmol/L) was significantly more than the group with lower sr. homocysteine(153.2±21.4 μmol/L) Serum LDL level in group with higher homocysteine (105.21±23.2 μmol/L) was significantly more than the other group (28.43±9.6 μmol/L). In a study by EL Oudi et al11. Acute coronary syndrome patients had significantly elevated levels of total homocysteine (P<0.01), HsCRP (P<0.001), IL-6 (P<0.001), TNFa (P<0.001), folates (P<0.05) and vitamin B12 (P<0.001), but lower high-density lipoprotein cholesterol (P<0.05) levels. Some clinical studies have shown that increasing dietary intake of vitamin B12 and folic acid has reduced the Homocysteine concentration and the risk of coronary artery disease.12
CONCLUSION Srhomocystein level in coronary artery disease patients was significantly higher than controls. Serum total cholesterol and serum LDL was significantly higher in hyperhomocysteinemia.
REFERENCES
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.