 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 2 - February 2019
Sonali Uttamrao Landge1*, Prafful V Jatale2, Vilas Kirdak3, Kaleem Shaikh4
1Assistant professor, 2NM Physician, 3Professor, 4Assistant Professor, 5SR, JIIUS Indian Institute of Medical Science and Research Medical College, Warudi, Tq. Badnapur, Dt. Jalna 431202, INDIA. Email: dr.jatalesp7@gmail.com
Abstract Background: Facial nerve is the longest nerve in a bony canal. Three dimensional anatomical knowledge provides the foundation for safe and skilful dissection of the very complex temporal bone and tortuous facial nerve. Objectives: This study aimed to see the variations of facial nerve in tympanomastoid segment course in 50 cadavaric temporal bone dissection in the tertiary care hospital. Material and Methods: The present cross observational study was carried out from October 2009 to October 2011. Preserved 50 temporal bones were obtained for the study and dissection was carried out on wet temporal bone in temporal bone laboratory. Modified radical mastoidectomy procedure was done. Lateral sinus plate, bony horizontal semicircular canal, digastric ridge exposed and identified. Facial nerve and its relations with the important middle ear structures and their anomalies with the help of various equipment was seen. Results: Out of 50 bones dissected, 44 (88%) bones were well pneumatised and 6(12%) bones were sclerotic. Length of the tympanic segment varied from 7.8-11.88 mm with a mean of 9.47 mm (±1.06mm). In 20 bones (40%) the length of the tympanic segment was 8.6-9.5 mm. The length of mastoid segment varied from 10 to 16 mm, with a mean of 13.59 mm (±1.27 mm. In 17 bones (34 %) length of the mastoid segment was 13.1-14 mm. The distance of second genu from outer cortex varied from 17.87 -23.67 mm with a mean of 19.64 mm (± 1.42 mm). The distance of second genu from outer cortex was 18.6-19.5 mm in 14 bones (28%) each. Distance of chorda tympani from stylomastoid foramina varied from 3.4-7.8 mm with a mean of 5.69 mm (±1.51mm). Conclusions: The study has provided knowledge of anatomy of temporal bone and its pneumatisation pattern, the anatomy of the facial nerve, its variations and their incidence, relation of various middle ear landmarks with the facial nerve and proficiency in dissection. Key Word: Tympanomastoid segment, Mastoidectomy, Facial nerve
INTRODUCTION Many facial expressions like joy, sorrow and other human expressions is a result of 7000 motor fibres of facial nerve firing in unison and a time. Facial nerve dysfunction causes disfigurement, emotional distress leading to detriment in social interaction. Inability to smile due to a surgeon’s faulty technique is an unforgivable crime. Only by cadaveric dissections can the aspiring ear surgeon learn to safely traverse the perilous anatomy of temporal bone so as to avoid injury to the many vital structures concealed in an area no larger than an olive.1 Throughout the era characterized by frequent operations for mastoiditis, one of the principle operative hazards was traumatic injury to the intratemporal segment of the facial nerve resulting in temporary or permanent facial paralysis. If the anatomical landmarks are followed and extra caution taken, iatrogenic injury to the facial nerve can be prevented. The facial canal, as it traverse the temporal bone, may display congenital bony dehiscence, variation, and anomalies in its usual course and in rare instance, may include a large persisting embryonic artery or vein. each of this feature can have clinical and surgical significance. The otologic surgeon wants to be familial with these variations and must suspect and identify them in order to avoid injury to the facial nerve.2 Temporal bones were dissected in the present study and length of various segments of facial nerve, its relation with middle ear structures and variations were noted.1 This study aimed to see the variations of facial nerve in tympanomastoid segment course in 50 cadavaric temporal bone dissection in the tertiary care hospital.
MATERIAL AND METHODS The Current study was conducted at Dept. Of E.N.T, Temporal bone lab in Department of Otolaryngology, JIIUS Indian Institute of Medical Science and Research Medical College, Warudi, Badnapur, Jalna. The present study was carried out from October 2009 to October 2011. Preserved 50 temporal bones were obtained for the study and dissection was carried out on wet temporal bone in temporal bone laboratory. Modified radical mastoidectomy procedure was done. Lateral sinus plate, bony horizontal semicircular canal, digastric ridge exposed and identified. Facial nerve and its relations with the important middle ear structures and their anomalies with the help of various equipments was seen. Under magnification simple mastoidectomy is performed first. Unroofing of epitympanum is done and the cells at the root of zygoma are exenterated. Up to this stage the postero superior meatal wall is intact. At this stage the landmarks were – posterior bony canal wall, tegmen plate, sigmoid sinus, incus, incudo malleolar joint, lateral semicircular canal dome and mastoid tip. The posterior canal wall is adequately thinned out. Then under higher magnification, the bridge is taken down. This procedure was done initially with cutting burr and finally with diamond burr. Once the bridge was taken down the further step was removal of anterior buttress. Anterior buttress removal was continued until there was a gradual curve from tegmen to anterior wall of external auditory canal without any projections or ridges. Then the posterior butterss was removed adequately. The ridge was then lowered up to the level of the floor of the external auditory canal. While lowering the facial ridge every precaution was taken not to injure the facial nerve. At the facial nerve are a the drilling was continued with continuous profuse irrigation. At this stage facial canal was visualized. The vertical segment of facial nerve was decompressed with the biggest possible diamond burr. Direction of the drill was parallel to the nerve with profuse irrigation. The bone over the anterior aspect of the 2nd genu was thinned keeping the direction of the burr parallel to the nerve. This prevented damage to semicircular canal. Incus and malleus were disarticulated and removed. Using a small diamond burr, the lateral and inferior bone of the horizontal segment of the facial canal was thinned. With the help of blunt dissector, the thinned bone over the dissected length of the facial nerve was removed. Care was taken not to damage the nerve sheath during this dissection. Different parameters were studied segment wise. Measurements were done by means of straight and curved caliper, and protractor.
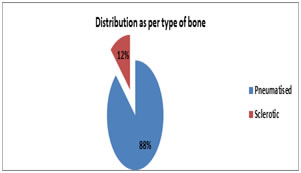
RESULTS Figure 1: Distribution as per type of bone Out of 50 bones dissected, 44 (88%) bones were well pneumatised and 6(12%) bones were sclerotic.
Table 1: Distribution as per length of tympanic segment
Length of the tympanic segment varied from 7.8-11.88 mm with a mean of 9.47 mm (±1.06mm). In 20 bones (40%) the length of the tympanic segment was 8.6-9.5 mm.
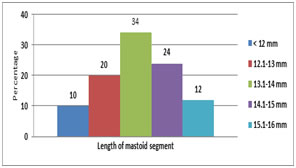
Figure 2: Distribution as per length of mastoid segment. The length of mastoid segment varied from 10 to 16 mm, with a mean of 13.59 mm (±1.27 mm). In all 50 temporal bones, the mastoid segment of facial nerve was anterior to the tip of mastoid and medial to tympanomastoid suture. In 17 bones (34 %) length of the mastoid segment was 13.1-14 mm, in 12 bones (24%) the length was 14.1-15 mm, while in 10 bones (20%) it was 12 -13 mm. In 6 bones (12%) it was 15.1-16 mm and <12 mm in 5 other bones (10%).
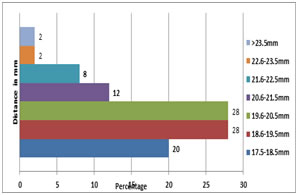
Figure 3: Distance of second genu from outer cortex The distance of second genu from outer cortex varied from 17.87 -23.67 mm with a mean of 19.64 mm (± 1.42 mm). The distance of second genu from outer cortex was 18.6-19.5 mm in 14 bones (28%) each. In 14 bones (28%) it was 19.6-20.5 mm. The angle between tympanic and mastoid segment varied between 95 degree to 125 degree with a mean of 109.2 degree (± 11.05 mm).
Table 2: distance of chorda tympani from stylomastoid forame
Distance of chorda tympani from stylomastoid foramina varied from 3.4-7.8 mm with a mean of 5.69 mm (±1.51mm). In 12 bones (24%) distance of chorda tympani from stylomastoid foramina was 4.1-5.0 mm, In 11 bones (22%) it was 7.1-8.0 mm, in 10 bones (20%) it was 5.1-6.0, in 9 (18%) bones it was 6.1-7.0 while in 8 (16%) bones it was 3.1-4.0 mm.
DISCUSSION In the present study of 50 temporal bones, 88% of bones were pneumatised and 12 % were sclerotic. This finding is concomitant with the literature. The high degree of pneumatization makes the dissection easier but may predisposed the individual to pneumatocele because the bones were very thin whereas the poorly pneumatised makes the dissection slower in other to avoid injury to underlying structure and also not to miss the landmark; however most of the structures like the facial nerve and it canals maintain their anatomic position despite the few marrow spaces. The mean length of tympanic and mastoid segment was found to be 9.47 mm ± 1.06 mm (range 7.8mm -11.88 mm), 13.59 mm±1.27(range 10 mm to 16 mm) respectively, which is considerably at variance to different cranial configuration of various races Below table explains the length of facial nerve segments of Japanese, Americans and Indian subjects. In the present study the length of tympanic segment varied from 7.5-11.88 mm with a mean length of 9.47mm (± 1.06mm). The minimum length noted was approximately 7.8 mm in 16 % of specimens. Minimum length of 7 mm has been noted by Agarwal et al3 and Kharat et al1 (2009) which was similar to the present study. The maximum length of the tympanic segment was approximately 11.5 mm (seen in 4% of specimens) in the present study which is similar to the maximum limit of length shown in the study of Kharat et al1, Wiet R J et al4 and Proctor B et al5. In all 50 temporal bones dissected, the tympanic segment of facial nerve turned posterior from geniculate ganglion. Tympanic segment of the nerve was found to lie above the oval window and below the horizontal semicircular canal, above and medial to processus cochleariformis and tensor tympani in all 50 specimens. Similar findings have been reported by most of the other authors. In the present study the length of mastoid segment varied from 10-16 mm with a mean length of 13.59 mm (± 1.27 mm). The minimum length noted was approximately 10 mm in 10 % of specimens. Minimum length of 7 mm has been noted by Agarwal et al3 so it is more than Agarwal et al3 study. Kharat et al1 showed minimum length 10 mm ,which was similar to the present study .The maximum length of the mastoid segment was approximately 16 mm ( seen in 12% of specimens ) in the present study which is similar to the maximum limit of length shown in the study Kharat et al1 , Wiet R J et al4 and proctor B et al5, In the present study the degree of descent was noted as 30 degree in all specimens , which is same as that noted by all the author s except Proctor B et al5, who showed degree of descent as 37 degree. Dehiscence of the bony facial canal in the horizontal segment within the middle ear entails a risk of immediate or delayed facial paralysis during middle ear surgery. The facial canal containing the facial nerve over the oval window was observed to show bony dehiscence in 12% by some authors and some workers reported dehiscence in the range of 6% to 70% Beddard D et al6. In the present study, out of 50 temporal bones dissections, dehiscence in the tympanic segment, were found in 2 bones. In 2 bones dehiscence was noted at tympanic segment. The incidence of dehiscence comes to 4%. The incidence is low as compared to most authors, but it is approximately similar with the study of Yadav SP et al7 and Kharat et al1. In all the 50 temporal bones tympanic segment of the facial nerve, turned posterior from the geniculate ganglion, the processus cochleaformis and tensor tympani were anterior to the nerve. The nerve passed above promontory and the oval window niche was inferior to the nerve. The nerve passed below the horizontal semicircular canal in all 50 temporal bones. In the present study, the distance of second genu from outer cortex varied from 17.87 mm with a mean of 23.67 mm (±19.64 mm). The range of distance of second genu from outer cortex in present study is concurrent with the study of Yadav SP et al7. Chorda tympani with Intratemporal origin have been found in the present study arise at a mean of 5.69 mm (range 3.4-7.8mm) proximal to the stylomastoid foramen. This distance from stylomastoid foramen was similar with corresponding mean distance of 5mm (range 1.0-11.0 mm) and 4.8mm (range 0-10 mm) fond by Nager GT et al8, and Muren C et al9 respectively. We agree with Wetmore SJ et al10 that the chorda tympani used as a landmark to identify the facial nerve in the mastoid by tracing it inferiorly to its origin. Over the year, the variations in the course of the mastoid segment of the facial nerve have become apparent. It does not always follow the vertical course as described in textbooks, but shows variations of surgical significance between the second genu and stylomastoid foramen. The bony architecture itself and the neurovascular structures in and around it make the temporal bone a difficult region to perform surgery. The localization of these important structures, such as the facial nerve and related surrounding relations in this bony framework might be challenging for the inexperienced surgeon. Therefore, the landmarks of the temporal bone with their relation among each other should be very well known. If the anatomical landmarks are followed and extra caution taken, iatrogenic injury to the facial nerve can be prevented.
CONCLUSION The variation among the values of each parameter consisting of the minimum and maximum measurements might be considered as a useful tool for choosing the best surgical approach during surgery. The variations occur with sufficient frequency as described in available literature, otologic surgeon must be aware of them, to avoid the disasters and the fear regarding facial nerve.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.