 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 3 - March 2019
A study of relationship between preoperative hearing and intraoperative findings in squamosal type of chronic otitis media
Ajit Lokare1*, Mukund Jadhav2, Koustubh Khandake3
1Professor and HOD, 2,3Senior Resident, Department of ENT, RCSM GMC, Kolhapur, Maharashtra, INDIA. Email: lokareajit@yahoo.com
Abstract Objectives: 1. To find out the percentage of erosion of each ear ossicles 2. To find out the most susceptible and most resistant ear ossicles for erosion in chronic otitis media of squamosal type. 3. To study the relationship between preoperative hearing loss obtained by the pure tone audiogram and ossicular erosion seen intra operatively. Materials and method: It was a retrospective observational study in tertiary care center. 30 patients with chronic otitis media of squamosal type who had undergone canal wall down mastoidectomy from January 2018 to December 2018 and were above 18 years of age were included. The patients who underwent CWDM for other indications were excluded. The data was collected from the patients during their routine postoperative follow up about their preoperative hearing and intraoperative findings from operative notes. Chi Square test was used to study the association between preoperative hearing and ossicular status seen intraoperatively. Results: Otorrhoea was the most common presenting complaint(100%) followed by hearing loss (80%). Malleus was eroded in 50%, absent in 10% and normal in 40% cases. Incus was eroded in 63.33%, absent in 30% and normal in 6.66% cases. Stapes was eroded in 40% with absent suprastructure and was found to be normal in 60% cases. Overall 28 patients (93.33%) had ossicular erosion or absence. Incus was the most commonly eroded ossicle that was eroded or absent in all these 93.33% cases.29 patients (96.66%) had cholesteatoma in middle ear, aditus and mastoid cavity involving separately or in all of them in extensive cases. Granulations were seen similarly in 20 cases (66.66%) in these regions. Cholesteatoma and granulations were seen to involve either alone or in combinations. The Chi square test showed no statistical association grade of hearing loss and erosion of malleus (p=0.121), incus (p=0.505) and stapes (p=0.240). Conclusion: Ossicular discontinuity is a common complication of chronic otitis media of squamosal type. Variable percentage of erosion of ear ossicles was observed. Incus was most susceptible ear ossicles for erosion in chronic otitis media of squamosal type and stapes was most resistant ossicle for erosion. This study couldn’t establish any definite association between preoperative hearing status and ossicular status seen intraoperatively. The poor association of preoperative hearing status with ossicular chain discontinuity in the presence of cholesteatoma may be due to the latter’s ability to transmit sound(i.e. cholesteatoma hearer). Key Word: chronic otitis media.
INTRODUCTION Chronic otitis media (COM) is a long-standing infection of a part or whole of the middle ear cleft. It manifests as ear discharge and deafness. Chronic otitis media is of two types squamosal (atticoantralor unsafe) and mucosal (tubotympanic/safe) type, with each of them having characteristic clinical features. The squamosal (atticoantral / unsafe) disease is often associated with a bone eroding entity such as cholesteatoma, granulations or osteitis and has the potential to cause life-threatening complications.1 Both types chronic otitis media may lead to erosion of the ossicular chain. This propensity for ossicular destruction is much greater incases of squamosal type chronic otitis media, due to the presence of cholesteatomaand granulations.2 The proposed mechanism for erosion is chronic middle ear inflammation as a result of overproduction of cytokines Tumor Necrosis Factor (TNF alpha), interleukin-2, fibroblastgrowth factor, and platelet derived growth factor, which promotehypervascularisation, osteoclast activation and bone resorption causing ossicular damage. TNF-alpha also produces neovascularisation and hence granulation tissue formation. However, the exact pathological mechanism of middle ear cholesteatoma is still unclear. Chronic otitis media is thus an inflammatory process with a defective wound healing mechanism.3 This inflammatory process in the middle ear is more harmful the longer it stays and the nearer it is to the ossicular chain.4 As middle ear ossicles form a part of the conducting apparatus for hearing. Any sort of pathology causing ear ossicles erosion may lead to ossicular discontinuity and thereby causing conductive hearing loss. An estimate of the ossicular damage due to any chronic ear pathology like chronic otitis media can be made with the help of a pure tone audiogram.5The final confirmation of the ossicular assembly status is intra-operative. A pre-operative ossicular assessment plays a very important role in the patient management in terms of type of procedure needed, extent of resection, prognosis and hearing outcome, need for any post-operative hearing rehabilitation and need for prosthesis (Total ossicular replacement prosthesis or partial prosthesis) and patient counselling.6 With this study we planned to study the relationship between the preoperative hearing and intara operative findings including ossicular status in squamosaltype of chronic otitis media.
AIMS AND OBJECTIVES
MATERIALS AND METHODS It was a retrospective observational study in tertiary care center. 30 patients with chronic otitis media of squamosal type who had undergone canal wall down mastoidectomy (CWDM) from January 2018 to December 2018 and were above 18 years of age were included. The patients who underwent CWDM for other indications were excluded. The data was collected from the patients during their routine postoperative follow up about their preoperative hearing and intra operative findings from operative notes. The data collected was tabulated in a systematic format and analyzed statistically. Chi Square test was used to study the association between preoperative hearing and ossicular status seen intraoperatively. SPSS version 25 for windows was used for statistical analysis. Assessment parameters
OBSERVATION AND RESULTS Age and sex distribution: All 30 patients were between 18-45 years and 50% were between the age 18-25 years. 17 were males and 13 were females. Distribution of symptoms
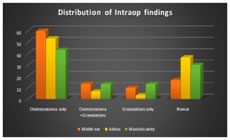
Otorrhoea was the most common presenting complaint, seen in all (100%) patients followed by hearing loss (80%), earache (26.66%) and tinnitus (13.33).Ear discharge was purulent, scanty, continuous and foul smelling in all cases. It was non-blood stained in 26 (86.66%) cases and blood stained in 4(13.33%) cases. Tympanic membrane findings: 20 patients (66.66%) had PSRP (Posterosuperior Retraction Pocket) and 13 (43.33%) had cholesteatoma flakes. Attic retraction was seen in 30% cases. Granulations over tympanic membrane were seen in 20% cases. Intraoperative findings: 29 patients (96.66%) had cholesteatoma in middle ear, aditus and mastoid cavity involving separately or in all of them in extensive cases. Granulations were seen similarly in 20 cases (66.66%) in these regions. Cholesteatoma and granulations were seen to involve either alone or in combinations with each other with distribution as shown in chart. Cholesteatoma alone was found in middle ear in 60% cases, in aditus in 53.33% cases and in mastoid cavity in 43.33% cases. Cholesteatoma with granulations was found in middle ear in 13.33% cases, in aditus in 6.66% cases and in mastoid cavity in 13.33% cases.
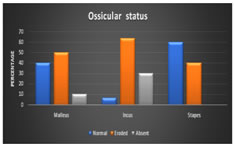
Intraoperative Ossicular status: Malleus was eroded in 50%, absent in 10% and normal in 40% cases. Incus was eroded in 63.33%, absent in 30% and normal in 6.66% cases. Stapes was eroded in 40% with absent suprastructure and was found to be normal in 60% cases. Overall 28 patients (93.33%) had ossicular erosion or absence. Incus was the most commonly eroded ossicle that was eroded or absent in all these 93.33% cases
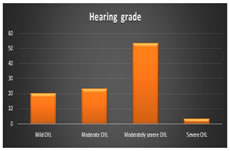
Preoperative grade wise hearing loss: Preoperatively most of the study population had moderately severe conductive hearing loss (53.3%) followed by moderate conductive hearing loss (23.3%) and mild conductive hearing loss (20%).
Preoperative Air Bone Gap (ABG): Majority of the patients had ABG of 40-60dB preoperatively consisting of 66.66%. 33.33% of patients had ABG between 26-40dB. Preoperative hearing loss & intraoperative status of ossicles: The association between the preoperative hearing loss and intraoperative ossicular status was studied for all the three ossicles. The number of patients in each grade of hearing loss were compared with status of each ossicle using Chi square test. The results for each ossicle are as given below. Table 1: Malleus
Table 2: Incus
The Chi square test showed no statistical association (p=0.505) between the erosion of incus and grade of hearing loss.
Table 3: Stapes
The Chi square test showed no statistical association (p=0.240) between the erosion of stapes and grade of hearing loss.
DISCUSSION 50% of our population was young adult population between 18-25 years and total 73.3% population was of less than 30 years. The mean age was 27.63 with std. deviation of 7.29. The mean age in the study by Ramazan o et al was 33.6 These findings were in fair agreement with those reported earlier by Salman et al. with most common age group 16–30 years.7 There was slight male predominance with male: female ratio of 1.3:1 compared to other studies of Asma A. et al(0.7), Ramazan O. et al (1.5:1) and Nafisa Parveen (1.7:1)8,9,10, The Right (14): Left16 ear ratio was 0.87 compared to study by Ramazan O et al. (0.7) and study by Nafisa Parveen (ratio 1)9,10 Otorrhoea was the most common presenting complaint (100%) followed by hearing loss (80%). This was consistent with the previous studies. On clinical examination and audiometry, all the patients were found to have a conductive hearing loss. Thus, otorrhoea and hearing loss were the clinical features of all the patients. 53.3% of them had moderately severe hearing loss and that was suggestive of extensive disease at the time of presentation. Most of the study population had long standing ear discharge for more than 10 years (26.66%) followed by those having for 6 to 10 years and for 2 to 5 years (23.33% each). This suggested chronic nature of disease in majority of the patients. Intraoperatively 29 patients (96.66%) had cholesteatoma in middle ear, aditus and antrum involving separately or in all of them in extensive cases and was the commonest intraoperative finding. This was consistent with previous studies by Asma A. et al (78%), Nafisa Parveen (76.7%) and Goyal et al(100%).8,10,11 Regarding distribution, cholesteatoma was seen in middle ear in 73.3% cases, in aditus in 60% cases and in antrum in 56.66% cases. Thus, middle ear was the commonest site of disease. This was against the studies by Palva12 and Asma A. et al8 which showed antrum to be the commonest site seen in more than 50% and 73% of cases respectively. Granulations were seen similarly in 20 cases (66.66%) either alone or with cholesteatoma in these regions. However, they were more common in antrum (26.66%) than in middle ear (23.33%). Overall 28 patients (93.33%) had ossicular erosion or absence and incus was the most commonly eroded ossicle that was involved in all these cases with or without other ossicles. It was eroded in 19 cases (63.33%) and absent in 9 cases (30%). This was consistent with many previous studies suggesting incus to be the commonest and earliest ossicle to get involved in cholesteatoma. Malleus was eroded in 15 (50%) cases and absent in 3(10%) cases. Stapes superstructure was absent in 40% cases. Most of the study population had moderately severe conductive hearing loss (53.3%) followed by moderate conductive hearing loss (23.3%), mild conductive hearing loss (20%) and severe conductive hearing loss (3.3%)preoperatively. This preoperative hearing was compared with intraoperative status of ossicles. In our study preoperative PTA showed that out of 15 patients with eroded malleus; maximum patients(11) had hearing loss of 56-70dB. 2 had hearing loss of 41-55 and other 2 patients had hearing loss of 24-40dB and >75dB. Out of 3 patients with absent malleus 2 had hearing loss of 56-70dB and one had hearing loss of 41-50dB. Out of 12 patients with intact malleus 5 had hearing loss of 26-40dB, 4 had 41-55dB and 3 had 56-70dB hearing loss. The Chi square test showed no statistical association between status of malleus and hearing loss with p value of 0.121 at df 6. Out of 19 patients with eroded incus, maximum9 had hearing loss of 56-70dB, 5 had 41-55dB, 4 had 26-40dB and one had >70dB hearing loss. Out of 9 patients with absent incus 7 had 56-70dB, 2 had 26-40dB and 41-55dB of hearing loss. Only 2 had absent incus who had hearing loss of 26-40dB and 41-55dB. The Chi square test showed no statistical association between status of incus and hearing loss with p value of 0.505 at df 6. Out of 12 patients with eroded stapes with absent superstructure, 8 had 56-70dB, 2 had 26-40 dB, 1 had 41-55dB and other 1 had >70dB hearing loss. Out of 18 patients with normal stapes, 8 had 56-70dB, 6 had 41-55dB and 4 had 26-40dB hearing loss. The Chi square test showed no statistical association between status of stapes and hearing loss with p value of 0.240 at df 3. There were 6 patients with mild conductive hearing loss. Out of them 1 had all the 3 ossicles eroded and 1 had incus and stapes eroded. Intraoperatively they had cholesteatoma connecting the eroded ossicles maintaining the conduction. Thus, they were cholesteatoma hearers. Goyal et al study of 140 patients with squamosal disease found that 5.71% of the patients had normal hearing sensitivity when cholesteatoma was found in all (100%) cases.11 Study by Albera et al observed Pure-tone audiometry and air-bone gap did not reflect actual ossicular chain status.13 Few clinical studies have carefully examined the relationshipbetween ossicular erosion by cholesteatoma and conductive hearing loss. Study by Jeng et al found that, in patients with cholesteatoma, preoperative ABG was not significantly correlated with ossiculardiscontinuity.14Carillo et al. expanded on Jeng’ swork by exploring the association of ossicular discontinuity with ABG cut off levels across different frequencies, and although the study found specific ABG cutoff valueswere associated with ossicular discontinuity in patients with chronic otitis media, no such association was foundin patients with cholesteatoma.15 In both studies, however, the status of the ossicular chain was evaluated and classified only as either continuous or discontinuous, with each study using slightly different criteria for what was considered is continuous. The poor association of audiograms in our study with ossicular chaindis continuity in the presence of cholesteatoma may be due to the latter’s ability to transmit sound i.e. Cholesteatoma hearers. Other factors, including the pars tensa surface area and ossicular fixation, can affect the hearing observed in patients with cholesteatoma. These factors were not directly measured in this study. Although ossicular evaluation is routinely performed intra operatively, prior knowledge of ossicular chain status gained from audiograms may influence the planned surgical technique and implications of treatment.
Ossicular discontinuity is a common complication of chronic otitis media of squamosal type. Variable percentage of erosion of each ear ossicles was observed. Incus was most susceptible ear ossicles for erosion in chronic otitis media of squamosal type andstapes was most resistant ear ossicle for erosion. This study couldn’t establish any definite association between preoperative hearing status and ossicular status seen intra operatively. The poor association of preoperative hearing status with ossicular chain discontinuity in the presence of cholesteatoma may be due to the latter’s ability to transmit sound(i.e. cholesteatoma hearer). Sample size was small to assess relationship of pure tone audiometry using statistical association. Other factors, including the pars tensa surface area and ossicular fixation, can affect the hearing observed in patients with cholesteatoma. These factors were not directly measured in this study, which was a limitation of this work.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.