 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
A study of diagnostic importance of ultrasound in first trimester bleeding
Darshana Legha1, Kamalpreet Singh2*
1Assistant Professor, 2PG, Department of Gynaecology, MMIMSR Medical College, Mullana (Ambala) Haryana, INDIA. Email: darshanalegha500@gmail.com
Abstract Background: Bleeding per vaginum in the first trimester is one of the most common obstetric problem. It is also one of the commonest causes for the majority of the emergency admissions and also common reason for ultrasound examination in the first trimester. Nearly 25% of all pregnant women in their first trimester complain of bleeding. Amis and objective: To study the diagnostic importance of ultrasound in first trimester bleeding. Materials and method: In the present study all pregnant women presenting with per vaginal bleeding during the first trimester were enrolled. All the selected cases were evaluated by using semi-structured questionnaire. A detailed history and comprehensive clinical examination including general, systemic, per abdomen and per vaginal examination were performed to arrive at a clinical diagnosis. Ultrasonoghraphy was performed in all the selected cases. Findings of clinical examination and ultrasonoghraphy findings were recorded. Results: On clinical examination threatened abortion was diagnosed in 82 cases whereas on ultrasonography 51 cases were confirmed to be of Threatened abortion. And disparity in diagnosis was observed in 31 cases. Disparity in case of complete abortion was 8 whereas in case of incomplete abortion was 2. In case of Blighted ovum disparity was observed in 10 cases. Out of total 107 cases of first trimester bleeding abortion was diagnosed in 100(93.46%) of cases, ectopic pregnancy was diagnosed in 5(4.67%) cases and hydatiform mole was diagnosed in 2(1.87%) cases. The sensitivity of clinical diagnosis in diagnosing viable intrauterine pregnancy was 100% but the specificity was 44.64%. Of the ectopic pregnancies diagnosed clinically, all were confirmed with sensitivity and specificity of100% and diagnostic accuracy of 100%. In diagnosing nonviable pregnancies, clinical diagnosis has got very poor statistical correlation with a sensitivity of 39.22%. Conclusion: Thus Ultrasonography has been proved as an important diagnostic modality in obstetrics. It is an easy available, diagnostic modality and it helps in the earlier diagnosis of complications of first trimester bleeding. In the above study it was demonstrated that it played an important part in diagnosis of first trimester bleeding. Key Word: first trimester bleeding, ultasonography, diagnostic importance
INTRODUCTION Bleeding per vaginum in the first trimester is one of the most common obstetric problem. It is also one of the commonest causes for the majority of the emergency admissions and also common reason for ultrasound examination in the first trimester. Nearly 25% of all pregnant women in their first trimester complain of bleeding.1,2 Usually, the patient will present with vaginal bleeding and mild-to-moderate subrapubic or midline lower abdominal pain that may radiate to the lower back.3 The clinician should ask about prior confirmation of pregnancy, last known menstrual period, when the bleeding began, quantity and character of bleeding, and current medications (ovulation agents put a woman at risk for a heterotopic pregnancy, which is an IUP and an EP simultaneously).4 The diagnostic workup of a women presenting with early pregnancy bleeding includes a complete blood count, WBC count with differential to rule out infection, urinalysis to rule out urinary tract infection, gonorrhea/chlamydia swab, Rh-type, qualitative β-hCG, transvaginal ultrasound, quantitative β-hCG, and serum progesterone levels.5,6,7 Currently, the TVUS and the quantitative β-hCG are considered first-line for diagnosis in early pregnancy bleeding.8 Data show that 91% of EPs are diagnosed with TVUS,9 which is preferred over transabdominal ultrasound because of increased sensitivity.5 Ultrasound (both trans-abdominal and transvaginal sonography) plays an important role in the evaluation of the causes of the first trimester bleeding, prognosticate and predict the status of abnormal pregnancy
MATERIALS AND METHOD The present cross-sectional study was conducted in the department of obstetrics and gynaecology of tertiary care institute for one year with the aim to study first trimester bleeding cases. Following inclusion and exclusion criteria was used to select the study subjects. Inclusion criteria:
Exclusion criteria:
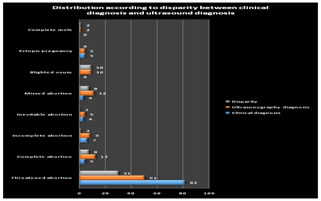
Thus by using the above mentioned inclusion criteria and exclusion criteria total 107 women with first trimester bleeding were included in the present study. The semi-structured questionnaire had been pretested amongst the randomly selected pregnant women with first trimester bleeding who meet the eligibility criteria for the study. From these results, questionnaire had been modified and validated for the entire study. A detailed history and a comprehensive clinical examination including general, systemic, per abdomen and per vaginal examination were performed to arrive at a clinical diagnosis. The patients were then subjected to ultrasound examination following which a definite management was planned. Trans abdominal scan (TAS) was done with sector probe 3.75 MHz frequency transducer. Transvaginal scan (TVS) using 6 MHz probe was done where findings of TAS were inconclusive. TVS was also done in early gestation and in all cases of suspected ectopic pregnancy. Prior to TAS, a full bladder was ensured. In ultrasound examination following findings viz., size of the uterus, presence of gestational sac, size and location of the gestational sac, gestational age compared to the period of amenorrhoea, whether the margins of the gestational sac are intact or crenated were noted. Foetal pole with crown rump length (CRL), cardiac pulsation, foetal movements and presence of fluid in the cul-de-sac were noted. Adnexa were scanned to rule out ectopic gestation and other pathology. Findings of clinical examination and ultrasonoghraphy findings were recorded. All responses were tabulated by the investigator using Microsoft-Excel 2007 Software. Graphical representations were made wherever necessary. RESULTS Table 1: Distribution according to disparity between clinical diagnosis and ultrasound diagnosis
Clinically threatened abortion was diagnosed in 82(76.64%) women whereas incomplete abortion was diagnosed in 7(6.54%) women. Complete abortion and ectopic pregnancy was diagnosed in 5(4.67%) cases each. On ultrasound threatened abortion was diagnosed in 51(47.66%) women. Complete abortion was diagnosed in 13(12.15%) women and missed abortion was diagnosed in 12(11.22%) women. Incomplete abortion was diagnosed in 9(8.41%) women respectively. On clinical examination threatened abortion was diagnosed in 82 cases whereas on ultrasonography 51 cases were confirmed to be of Threatened abortion. Thus in total 31 cases disparity was observed. Disparity in case of complete abortion was 8 whereas in case of incomplete abortion was 2. In case of Blighted ovum disparity was observed in 10 cases.
Table 2: Causes of bleeding per vaginum in the first trimester of pregnancy
Out of total 107 cases of first trimester bleeding abortion was diagnosed in 100(93.46%) of cases, ectopic pregnancy was diagnosed in 5(4.67%) cases and hydatiform mole was diagnosed in 2(1.87%) cases.
Table 3: Diagnostic importance of clinical examination in first trimester bleeding
Table4: Sensitivity, Specificity, Positive predictive value and Negative predictive value
The sensitivity of clinical diagnosis in diagnosing viable intrauterine pregnancy was 100% but the specificity was 44.64%. The accuracy of clinical diagnosis was 71.028% in diagnosing the viable intrauterine pregnancy. Of the ectopic pregnancies diagnosed clinically, all were confirmed with sensitivity and specificity of100% and diagnostic accuracy of 100%. In diagnosing nonviable pregnancies, clinical diagnosis has got very poor statistical correlation with a sensitivity of 39.22%, specificity of 100%, NPV 64.36% and accuracy of 71.028%.
Table 4: Clinical diagnosis Vs Ultasonography diagnosis
It was seen that out of 82 cases clinically diagnosed as threatened abortion, only 51 cases were continued as live pregnancy. Whereas rest of 31 cases were misdiagnosed clinically and out of them 8 were diagnosed as complete abortion, other 8 were of missed abortion, 10 cases were of blighted ovum. Incompetent abortion and complete mole was confirmed in 2 cases each whereas one case was of inevitable abortion. No case of blighted ovum and complete mole was diagnosed clinically. 5 cases of ectopic pregnancy diagnosed clinically were confirmed as ectopic pregnancy on ultrasound.
DISCUSSION The present study was conducted in the department of obstetrics and gynaecology with the aim to study the first trimester bleeding and to correlate the clinical findings with Ultrasonography. It was seen that clinically threatened abortion was diagnosed in 76.64% women whereas incomplete abortion was diagnosed in 6.54% women. Complete abortion and ectopic pregnancy was diagnosed in 3.74% cases each. Thus threatened abortion was the most common finding on clinical examination. Gawade S et al10 observed threatened abortion as the most common clinical diagnosis (86.67%) in patients presenting with first trimester bleeding per vaginum. Other cases were diagnosed as missed abortion (5.33%), incomplete abortion (4.0%), ectopic pregnancy (2.0%), hydatiform mole (0.67%), threatened abortion with cervical polyp (0.67%) and complete abortion (0.67%). Similar findings were also reported by Asha Hanamshetty et al11, Mamatha Shivanagappa et al12 and S. Sujatha et al13, Damania et al14 and Chaudhary et al15. Ultrasonography was performed in all the women in the study and threatened abortion was confirmed in 47.66% women. Complete abortion was diagnosed in 12.15% women and missed abortion was diagnosed in 11.22% women. Incomplete abortion was diagnosed in 8.41% women respectively. Gawade S et al10 reported that on ultrasonography threatened abortion was the most common diagnosis (44%) followed by missed abortion (22%). Blighted ovum was a new diagnosis in 12.67% of cases which cannot be diagnosed by clinical methods. The findings of the present study were also comparable with the findings observed by Asha Hanamshetty et al11, Mamatha Shivanagappa et al12 and S. Sujatha et al13 in their study. It was observed that threatened abortion was diagnosed in 82 cases on clinical examination whereas 51 cases were confirmed to be of threatened abortion on ultrasonography. Thus in total 31 cases disparity was observed. Disparity in case of complete abortion was 8 whereas in case of incomplete abortion was 2. In case of Blighted ovum disparity was observed in 10 cases. Gawade S et al10 in their study observed that 86.67% cases were clinically diagnosed as threatened abortion whereas only 50.77% cases had similar diagnosis on ultrasound with a discrepancy of 49.23%. Mamatha Shivanagappa et al12 observed 94 cases of Threatened abortion clinically whereas in 46 cases the diagnosis was confirmed on ultrasonoghraphy thus the disparity was observed in 48 cases. Asha Hanamshetty et al11 and S. Sujatha et al13 also observed similar findings in their study. In present study, various abortions contributed to a major chunk of first trimester bleeding constituting 93.46% with ectopic pregnancy and H Mole making up the rest of the cases with frequencies of 4.67% and 1.87% respectively, when compared with P. Reddi Rani et al16 and Rama Sofat et al17. Mamatha Shivanagappa et al12 in their study reported that abortion was a major cause of the first trimester bleeding constituting 83%. The incidence of ectopic pregnancy was 13% and the incidence of mole was 4%. In the report by Rani et al16, also abortion was the leading cause with an incidence of 61%. The subjects in the study group were divided into three main categories for the purpose of statistical correlation i.e. viable intrauterine pregnancy, non-viable intrauterine pregnancy and ectopic pregnancy. The sensitivity of clinical diagnosis in diagnosing viable intrauterine pregnancy was 100% but the specificity was 44.64%. The accuracy of clinical diagnosis was 71.028% in diagnosing the viable intrauterine pregnancy. Of the ectopic pregnancies diagnosed clinically, all were confirmed with sensitivity and specificity of 100% and diagnostic accuracy of 100%. In diagnosing nonviable pregnancies, clinical diagnosis has got very poor statistical correlation with a sensitivity of 39.22%, specificity of 100%, NPV 64.36% and accuracy of 71.028%. Mamatha Shivanagappa et al12 in their study observed that out of 94 cases of suspected viable intrauterine gestation on clinical examination 46 cases were confirmed which showed the sensitivity of 82%, specificity of 52%, PPV of 40%, and NPV of 88%. Of the 9 ectopic pregnancies diagnosed clinically, all were confirmed with specificity of 100%, PPV of 100%, and NPV of 92%. In diagnosing non-viable pregnancies, the clinical diagnosis had a very poor statistical correlation with sensitivity of 50%, specificity of 81%, PPV of 62%, and NPV 72%. Thus the fings were comparable with the present study. In the present study it was seen that out of 82 cases clinically diagnosed as threatened abortion, only 51 cases were continued as live pregnancy. Whereas rest of 31 cases were misdiagnosed clinically and out of them 8 were diagnosed as complete abortion, other 8 were of missed abortion, 10 cases were of blighted ovum. Incompetent abortion and complete mole was confirmed in 2 cases each whereas one case was of inevitable abortion. No case of blighted ovum and complete mole was diagnosed clinically. 5 cases of ectopic pregnancy diagnosed clinically were confirmed as ectopic pregnancy on ultrasound. In study by Gawade S et al10 threatened abortion was clinically diagnosed in 130(86.67%) cases. Amongst these, only 66(50.77%) cases were confirmed as threatened abortion by ultrasound. Remaining 64(49.23%) cases clinically diagnosed as threatened abortion were diagnosed as missed abortion 28(21.54%), blighted ovum 16(12.31%), incomplete abortion 8(6.15%), ectopic pregnancy 6(4.62%), hydatiform mole 3(2.31%) and complete abortion 3(2.31%) on ultrasonography thereby emphasizing a crucial role of ultrasound in confirming clinical diagnosis of patients with first trimester vaginal bleeding. Amongst the 8(5.33%) cases clinically diagnosed as missed abortion, 5(62.5%) cases were actually missed abortion and the remaining 3(37.5%) were blighted ovum on ultrasound. Also, amongst the clinically diagnosed 6 cases (4%) of incomplete abortion, only 1 case (16.67%) turned out to be incomplete on ultrasound and rest 5 cases (83.33%) were complete abortions thereby indicating the superiorority of ultrasound in confirming clinical diagnosis. Further, one case diagnosed as complete abortion was found to be ectopic pregnancy on ultrasound. Cases clinically diagnosed as ectopic (2%), hydatiform mole (0.67%) and threatened abortion with cervical polyp (0.67%) correlated well with ultrasound diagnosis. Jaideep Maihotra et al18 in his prospective evaluation of 150 patients with first trimester bleeding found that ultrasonography helped in establishing the correct diagnosis in 32% of clinically misdiagnosed cases. He concluded that ultrasonography was the only imaging modality, by which an accurate assessment of first trimester bleeding can be done from the diagnostic and prognostic point of view. Sofat et al17 compared and correlated clinical diagnosis and ultrasound diagnosis. They found that ultrasound had a definite edge over clinical diagnosis. Thus to summarize, in this study, the causes of bleeding covered a spectrum of conditions ranging from a viable pregnancy to non-viable pregnancy. Ultrasound examination was a good indicator for evacuation in cases of abortion. Using ultrasound, pregnancy with higher chances of a viable birth could be differentiated from a pathological pregnancy warranting an immediate termination. The earlier concept was that nothing is better than the two fingers of an obstetrician, but today ultrasound has been shown to have a definite edge. Ultrasound is aptly described as the third finger of the obstetrician.
CONCLUSION Thus we conclude that as compared to ultrasonography, clinical examination has less accuracy in diagnosing the viable intrauterine pregnancy. Clinical diagnosis has equal diagnostic accuracy in diagnosing ectopic pregnancies as compared to USG. In diagnosing nonviable pregnancies, clinical diagnosis has got very poor accuracy as compared to USG. Thus Ultrasonography has been proved as an important diagnostic modality in obstetrics. It is an easy available, diagnostic modality and it helps in the earlier diagnosis of complications of first trimester bleeding. In the above study it was demonstrated that it played an important part in diagnosis of first trimester bleeding.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.