 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 - November 2019
Iliopsoas abscess as a cause of puerperal sepsis
Aakanksha Mahajan1*, Ishan Gupta2, Kavita Choudhary3
1,3Senior Resident, Department of Gynaecology, Lady Hardinge Medical College, Delhi University, New Delhi, INDIA. 2Senior Resident, Government Medical College Jammu, University of Jammu, Jammu, J and K, INDIA. Email: aakankshamjn@gmail.com
Abstract Iliopsoas abscess is an uncommon cause of sepsis with an incidence of 0.4 cases per 100,000 population per year. This clinical problem may occur as a postpartum complication rarely but a delay in diagnosis is common because of its insidious development and lack of specific symptoms and signs. This article aims at reviewing the etiopathogenesis, the presentation, diagnosis and management of this unusual case. Making the obstetricians aware about this underdiagnosed disease can decrease the high morbidity and mortality associated. Key Words: infection, postpartum, iliopsoas, abscess, diagnosis.
INTRODUCTION Iliopsoas abscess is an uncommon phenomenon with an incidence of 0.4 cases per 100,000 population per year.1 It is a disease that can produce vague clinical characteristics, causing difficulty in its diagnosis 2. Obstetricians are usually familiar with predictable signs and symptoms of post partum sepsis. However infections of paracervical and paravertebral structures may produce a confusing clinical picture and may spread to involve tissues of pelvic side wall further complicating the picture 3. The diagnosis may be a particular challenge because pain in the lower back and buttocks is common and often nonspecific during pregnancy and the postpartum period. Since the first description of psoas (or iliopsoas) muscle abscess by Herman Mynter in 1881,4 this infection has been recognized as infrequent, insidious, misdiagnosed, and a potentially life-threatening condition. CLINICAL PRESENTATION The clinical presentation of iliopsoas abscess is insidious and non-specific, and thus may pose a diagnostic challenge for clinicians. The classic triad of fever, pain and limp may not be present and initial misdiagnosis is common 5. The patient may present with one sided lower abdominal pain radiating to the anterior aspect of the upper part of the thigh, or with severe back ache. Fever, rigors and vomiting may also be associated, although not necessarily. Patient may also have urinary complaints like dysuria, urgency or increased frequency of micturition. It is important to illustrate the history of tuberculosis, HIV, diabetes, renal problems, trauma. A careful neurological examination is also required to rule out any paresthesia. On examination, swelling or induration localized to the site of abscess may be evident. Raised local site temperature, guarding, rigidity, tenderness may or may not be present. The psoas sign—a worsening of lower abdominal pain on the affected side with passive extension of the thigh while supine may be present. The patient may hold the hip in flexion to relieve pain. A lump may be present at the groin. Per speculum examination visualizes the cervix and vagina for evidence of any abnormal bleeding or discharge. Bimanual vaginal examination reveals the size; position of the uterus, whether anteverted or retroverted and whether any adnexal tenderness or masses are present.
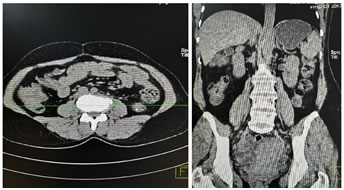
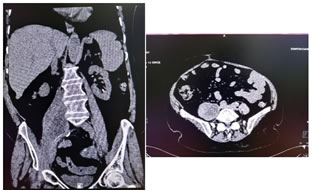
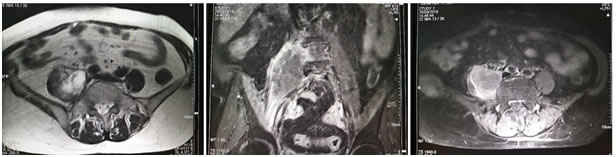
DIAGNOSIS Investigations include complete blood count, differential count, C reactive protein, ESR, urine routine and culture, blood culture, renal and liver function tests, vaginal and endocervical swabs. Ultrasound is the first line investigation for radiological diagnosis, however the diagnosis is often missed because of lack of clinical suspicion. Even with clinical suspicion, it is diagnostic in only 60% of cases 6. Sonography is also essential to rule out the evidence of any retained products of conception. Simple abdomen radiography can demonstrate blurring of the psoas muscle region, and air enhancing duodenal or renal contour, although its diagnostic value for psoas abscess is restricted . The sacroiliac joint, the lumbar spine, and intervertebral disks should be carefully examined. If a lesion is too small to reveal soft tissue gas, spinal destruction, mass effects or unusual iliopsoas, plain films would only reveal negative findings 7. CT is the most accurate investigation for diagnosis of iliopsoas abscess with reported sensitivity of 100% and specificity of 77% 8. Few studies state that the magnetic resonance imaging (MRI) can differentiate soft tissues more accurately, producing a clear view of the abscess wall and its surrounding structures without the use of a radiocontrast agent, thus, making the MRI a better choice than the CT scan 9. On CT scans, an abscess may manifest as enlargement of the iliopsoas muscle by a low-attenuation lesion [FIG 1, FIG 2]. The lesion typically displays rim enhancement after the intravenous administration of contrast material . Abscesses appear as areas of low signal intensity at nonenhanced T1-weighted MR imaging and as areas of high signal intensity at nonenhanced T2-weighted MR imaging [FIG 3]10. Secondary findings include obliteration of the surrounding fascial planes, bone destruction, and gas bubbles. CT is more sensitive than MR imaging for demonstrating gas bubbles.11 Figure 1 Figure 2 Figure 3 Figure 1: Coronal and Axial CT images showing normal appearance of bilateral psoas muscles which show uniform attenuation and well defined margins; Figure 2: Non contrast axial and coronal CT images showing right psoas abscess; Figure 3: T2w axial and post contrast T1FS axial and coronal images showing right psoas abscess
Bone scans should be carried out if plain CT films show negative or unverifiable results. Furthermore, bone scans are useful and important for detecting unexpected concomitant infectious foci, especially in patients with pyrexia of unknown origin 12.
MANAGEMENT Treatment should be started as soon as a clinical diagnosis of psoas abscess is confirmed. The administration of appropriate antibiotics and prompt surgical drainage are necessary. Antibiotics, based on culture sensitivity report given for 3–4 weeks are usually sufficient for patients without complications. Tubercular lesions must be treated with the appropriate antituberculous regimens 5. Both Ultrasound and CT imaging modalities allow for earlier detection and enable therapeutic drainage to be performed. CT-guided percutaneous drainage is technically similar to open surgical drainage and has been advocated as the drainage method of choice 13.
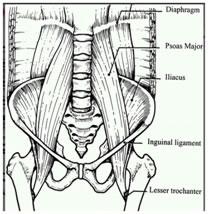
DISCUSSION In obstetrical practice, postpartum infection usually involves the uterus and adjacent pelvic structures presenting with typical and predictable symptoms and signs. However, musculoskeletal and focal neurological infections can rarely be seen in the postpartum period 14. The iliopsoas compartment consists of the psoas major, psoas minor, and iliacus muscles. The psoas muscle is the main flexor of the thigh, although it also flexes the trunk over the hip. Its proximal insertion is on the anterior surface of the transverse processes of all lumbar vertebrae, the lateral margin of the vertebral body of multiple vertebrae (T12 to L5), and the intervertebral disc between them. Its distal insertion is at the lesser trochanter of the femur. It merges with the iliacus muscle at the level of the L5 through S2 vertebrae to form the iliopsoas muscle (FIG 4) 15.
Superiorly, the psoas muscle passes beneath the arcuate ligament of the diaphragm; therefore, it is a potential channel for communication between the mediastinum and the upper thigh. Inferiorly, there is a potential communication between the iliopsoas compartment and the posterior pararenal space. Anteriorly, the psoas muscle is closely related to the pancreas, aorta, inferior vena cava, and retroperitoneal lymph nodes. Structures such as the duodenum, cecum, and appendix in the right side of the abdomen and the descending colon in the left side of the abdomen are close to the iliopsoas compartment. Violation of the retroperitoneal fascial planes by infective, hemorrhagic, and neoplastic processes may give rise to lesions within this compartment 11.For this reason, infections of intra-abdominal organs can spread to the iliopsoas muscle. The important blood supply of this muscle is supposed to predispose it to hematogenous spread from occult sites of infection 16.Psoas abscess is classified into primary or secondary depending on the etiology. Primary iliopsoas abscess usually originates through hematogenic dissemination. Its known causes are many, although Staphylococcus aureus, Escherichia coli, Bacteroides sp., Mycobacterium tuberculosis, Streptococcus viridans, Enterococcus faecalis, and Peptostreptococcus are the most common source of infection. Immunosuppressed patients have a higher risk of developing this disease 17.Secondary Psoas abscess, on the other hand, is more common in adults over 50-years-old, and originates through infections from adjacent sites, for example: the gastrointestinal tract (Escherichia coli and other Enterobacteria), and the vertebral column (Mycobacterium tuberculosis) etc 18.Tuberculosis of the spine is the most common and most dangerous form of tuberculous infection and an early diagnosis is required as delay in diagnosis and management causes spinal cord compression and deformity and may lead to paraplegia or quadriplegia depending on the site involved 19. Pregnancy is a immunocompromised state which may predispose the patient to infections. Trauma during delivery may also cause a haematoma in the iliopsoas muscle which subsequently may become infected . Another possibility is the disruption of the sacroiliac joint during delivery that may result in a retroperitoneal abscess 20. Shahabi et al. found that vaginal or cervical lacerations could potentially spread retroperitoneally causing an abscess 21. In addition, transient bacteremia following pharyngitis or urinary tract infection may predispose patients to this condition 3. Clinical picture presents a diagnostic challenge. A careful history and close examination of the patient is of crucial importance. The more familiar causes of postpartum sepsis like endometritis, retained products of conception or urinary tract infections should be ruled out first. It is also very important to rule out the evidence of any deep venous thrombosis. The typical triad of fever, lumbago, and restriction of the hip movement is present in only 30% of cases22. As the psoas muscle is innervated by L2–L4, pain can radiate to hip and the lower extremity, mimicking the sciatic nerve symptom of pain. Indeed, there is a direct anatomical link between the psoas muscle and surrounding neural structures (lumbosacral structures) that can produce radicular pain 23. If the pus tracks down along the muscle it passes downwards beneath the inguinal ligament and may present as a lump in the groin area. Only 13% of patients with iliopsoas abscess may have a palpable mass on physical examination24. The psoas sign has a sensitivity of only 24% for iliopsoas abscess; it can also indicate inflammation to the iliopsoas muscle in other conditions such as retrocecal appendicitis25. Hip flexion deformity can be a helpful diagnostic feature, as 96% of patients with iliopsoas abscess hold the hip in flexion to relieve pain. But pain on hip flexion can also occur in conditions such as septic arthritis 26. Also collection of pus in the psoas muscle compartment may present with a gradual onset of symptoms, moderate pain, and low-grade or absent fever leading to a diagnostic dilemma. Laboratory tests reveal nonspecific signs of inflammation: marked elevation of the erythrocyte sedimentation rate and CRP levels, an increased peripheral white blood cell count, and occasionally anemia. Blood cultures may be positive for a particular organism causing the abscess. HIV test is recommended, as this is a cause for immunosuppression predisposing to the development of iliopsoas abscess. In endemic areas, every effort should be made to ensure that the mycobacterium is excluded by acid-fast staining and culture techniques 27. Modern imaging techniques such as ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI) and radionuclide scans, allow more rapid diagnosis and decrease the morbidity and mortality of patients with psoas abscess 7. Ultrasound is first line radiological tool used although computed tomography is effective for diagnosis and allows percutaneous drainage of the abscess. Psoas abscess can be associated with other diseases, including: Crohn’s disease, diverticulitis, appendicitis, colorectal cancer, urinary tract infection, vertebral osteomyelitis, septic arthritis, sacroiliitis, abdominal aortic aneurysm, endocarditis, and suppurative lymphadenitis 22. The long-term morbidity of an untreated iliopsoas abscess includes femoral nerve compression and the abscess tracking into the hip joint leading to a septic arthritis and possible osteomyelitis. The disability from such complications is high 28.
CONCLUSION The possibility of psoas muscle abscess should be taken into differential diagnosis when investigating a case of puerperal sepsis. Poorly characterized in its etiology and clinical associations, an infectious emergency of this type usually presents in a nonspecific manner and poses a significant diagnostic challenge, leading to an underdiagnosed disease with high mortality rates. Computed tomography is effective for diagnosis and allows percutaneous drainage of the abscess . Correct and fast identification of the microorganisms in addition to appropriate usage of antibiotic regimen and surgery improves the outcome. Morbidity and mortality can be reduced with early detection and hence a high degree of clinical suspicion should be maintained in a patient with an unexplained cause of postpartum sepsis.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.