 Home
Home
|
Table of Content - Volume 13 Issue 3 - March 2020
A study of various factors that affect TOLAC (trial of labour after caesarean) after previous one caesarean section
Pradeep Patil1*, Vrunda Choudhary2
1,2Assistant Professor, Department of Obstetrics & Gynecology, Ashwini Rural Medical College, Hospital and Research Center, A/P - Kumbhari, Tal. South Solapur, Dist.- Solapur, Maharashtra, INDIA. Email: mmpateltrust@gmail.com
Abstract Background: Women undergoing cesarean section have a higher morbidity and mortality rate than those having vaginal birth. Complications associated with caesarean section are postpartum hemorrhage, need for blood transfusion, anesthesia-associated complications, surgical risks like intestinal obstruction, wound dehiscence, wound scars, infection, etc. TOLAC (Trial of Labour Aafter Caesarean section) reduces above risk. Aim and objective: To study the various factors that affect Trial of Labour After one caesarian section Methodology: Total 261 patients were studied in department of Obstetrics and Gynaecology. Data included sociodemographic data and maternal factors related to VBAC like Age, Education, Parity, Gestational age, Registered / unregistered pregnancy, lndication for previous LSCS, Lower uterine segment thickness on USG, Spontaneous or lnduced Labor, Cervical dilatation at the time of admission to labor room. Trial of labour was given in labour rooms to those who have undergone spontaneous labour or who have been induced. Careful monitoring of labour was done partogram and fetal heart sound. Patients who required caesarean section were shifted to operation theatre. Remaining delivered by normal vaginal delivery or assisted delivery. Data was analysed with appropriate statistical tests. Results and discussion: Total 261 patients were given trial of labor. Out of those 193 patients (74%) delivered vaginally. This association of failed trial with cervical dilatation was statistically extremely significant. Education, gestational age, registration status of mother were statistically not significant. Key Word: TOLAC
INTRODUCTION Cesarean delivery is one of the most commonly performed operations today. As medical science and especially obstetrics has evolved over the recent years, there has been a parallel and steady increase in the rate of cesarean births. The operation of 'cesarean delivery' has also witnessed this evolution; from it being done in desperate situations as a postmortem surgery to save the unborn child to the present times when one of the most common indications for cesarean delivery is a previous cesarean birth. The advent of cesarean delivery was followed immediately by dilemmas in the management of the patient who had a history of a previous cesarean section. The introduction of the low transverse uterine incision by Kerr' in 1926 1was the largest boost for the advocates of vaginal birth after cesarean in the early decades of 1900s. Case2 explained that the 'Kerr' incision prevented peritonitis by limiting the seepage of infected material from the wound into the peritoneal cavity and thus lowered maternal mortality and morbidity. Merrill and Gibbss 3 reported from the University of Texas at San Antonio that subsequent vaginal delivery was safely accomplished in 83% of their patients with prior cesarean deliveries. This rekindled interest in VBAC (vaginal birth after cesarean delivery) at a time when only 2% of American women who had previously undergone cesarean section were attempting vaginal delivery. Aim and objective: To study the various factors that affect Trial Of Labour After one caesarian section
MATERIAL AND METHODS Present study was a prospective study. It was carried on 261 patients at a tertiary health care center. Patients admitted in department of obstetric and gynecology for delivery with history of one previous caesarian section were studied. lnclusion criteria: 1. Patients with only one previous caesarean 2. All vertex presentations 3. Singleton gestations Exclusion criteria: 1. Patients with known classical or inverted T incision during previous caesarean section. 2. Lower vertical scar in previous section 3. Patients with presentations/lie apart from vertex 4. Patients with multiple gestation 5. Patients having upper segment hysterotomy scar or Patients having previous scar of myomectomy. Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. Data collected with pre tested questionnaire. Data included sociodemographic data, various maternal factors like Age, Education, Parity, Gestational age, Registered / unregistered pregnancy, lndication for previous LSCS, Lower uterine segment thickness on USG, Spontaneous or lnduced Labor , Cervical dilatation at the time of admission to labor room, Cervical effacement at the time of admission to labor room, Station at the time of starting of trial. Patients who were registered during antenatal visits and patients who visited in emergency were studied. Lower uterine segment thickness was measured by ultrasound examination in patients after they have completed 36 weeks of gestation. But lower uterine segment thickness was not done in those patients who were in labour though have passed their 36 weeks of gestation. Pelvic Assessment was done to assess the adequacy of pelvis. Emergency preparedness measures like availability of surgeon, anaesthesia provider, operating room personnel and sufficient blood was always ensured. Trial of labour was given in labour rooms to those who have undergone spontaneous labour or who have been induced and labour augmentations by Pitocin in lV drip was done in those who required. Careful monitoring of labour was done by recording maternal pulse, Blood Pressure and plotting the partogram for each patient for cervical dilation and fetal Heart monitoring by intermittent auscultation by stethoscope and Doppler. Vigilant watch was kept for symptoms and signs of scar dehiscence such as maternal and fetal tachycardia, hypotension, fetal bradycardia, per vaginal bleeding; lower uterine segment tenderness or change in uterine contour especially when labour was induced or augmented. Patients who developed fetal distress, who crossed the action line on partogram, who developed signs and symptoms of scar dehiscence were shifted for emergency LSCS. Outcome of the pregnancy noted. Data analysed with appropriate statistical tests.
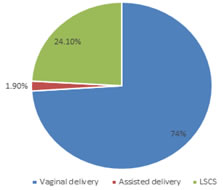
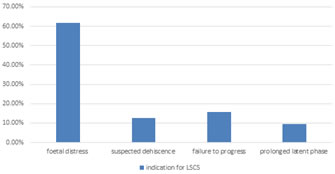
RESULTS Total 261 patients were given trial of labor. Out of those 193 patients (74%) delivered vaginally without assistance while only 5 patients (1.9%) required assistance with forceps. About 63 (24.2%) patients required repeat cesarean section.(fig 1) Most of the patients 149(57.08%) were in age group 20-25 yrs followed by 25-30 yrs 78(29.88%). Only 28(10.72%) patients were above 30 yrs of age. The need for repeat cesarean section was more in 20-25 yrs age group 282% 42 (16.09%) followed by in 25-30 yrs 20(7.66%). Only 1 patient above 30 yrs of age required repeat C.S. There was highly significant rate of vaginal delivery in patients above 30 yrs of age. The patients were distributed with rising trend when associated with level of education. Most of the patients were having above school level of education. The need for repeat cesarean section was increasingly present in patients having higher education. Most of the patients were registered at study place. (75%) while patients who were admitted in emergency were only 17.24%. But need for repeat C. S. was more in registered patients in comparison with unregistered patients i.e.21.45% Vs 2.68%. Registration status and mode of delivery were significantly not associated(p>0.05) .(table2) Lower uterine segment thickness was measured in 176 patients. lt could not be measured in 85 patients because most of them got admitted in active labor. lntraoperative finding of uterine dehiscence was present in only 2 patients these patients were not included in the study. Another important finding was that none of the patients with Lower uterine segment thickness <2.5 mm had uterine dehiscence.(table 3) When distributed according to gestational age most of the patients were in group 37 to 40 wks. About 55 patients were having gestation more than 40 weeks. More no. of patients required repeat C.S. as the gestational age went on increasing. Though this fact remained statistically insignificant when groups were compared among themselves. No. of the patients (n= 114) admitted in active phase of labor was slightly less than those admitted while not in active labor (n= 147). The need for repeat C.S was negligible in women having active labour at the time of admission to labor room i.e.2.68% when compared with another group i.e.21.45%. This association of failed trial with cervical dilatation was statistically extremely significant (table 4). When distributed according to gestational age most of the patients were in group 37 to 40 wks. About 55 patients were having gestation more than 40 weeks. More no. of patients required repeat C.S. as the gestational age went on increasing. Though this fact remained statistically insignificant when groups were compared among themselves.(table 5) Most of the patients who needed repeat C.S. were shifted because they developed fetal distress i.e.61% (n= 39) while 10 patients needed repeat C.S. because they failed to progress in labor accounting for 15.8%. Suspected dehiscence was indication in 8 patients while 6 patients had their latent phase of labor prolonged.(fig 2)
Figure 1: Mode of delivery
Table 1: Distribution of patients according to education of mother and type of delivery
Table 2: Distribution of patients according to registration status of mother and type of delivery
P=0.095 RR=0.87 (0.75-1.01)
Table 3: Distribution of patients according to Lower Uterine Segment thickness and type of delivery
Table 4: Distribution of patients according to cervical dilatation in mother and type of delivery
Table 5: Distribution of patients according to gestational age and type of delivery
p>0.05 not significant Figure 2: Distribution of patients according to indication for LSCS DISCUSSION The overall success rate of VBAC in our study was 74%. Various other study shows comparable results like Rageth et al. 4 73.3%, Sims et al. 5 77%, Elkousy et al. 6 74% and Bujold et al. 7 78 %. The success or failure, as in the cases of the present study, cannot be, thereby, attributed to the presence of a scar alone, but to the labour various maternal characteristics collectively, which precedes the repeat C.S. The repeat C.S. results due to failure of this labour. When distributed according to gestational age most of the patients were in group 37 to 40 wks. About 55 patients were having gestation more than 40 weeks. More no. of patients required repeat C.S. as the gestational age went on increasing. Though this fact remained statistically insignificant when groups were compared among themselves. Callahan et al., 8 in a case- control study, compared women attempting VBAC past 40 weeks of gestation with women of the same gestational age with no history of prior cesarean delivery. Among the cases, the VBAC success rate was similar to that reported in the literature (66%), but the choice of a comparison group without a history of prior cesarean limits the application of the study results to patient counseling. Zelop et al. 9 compared women attempting VBAC at or before 40 weeks of gestation with those attempting VBAC beyond 40 weeks. This study included 2,775 women, of whom 1,271delivered after 40 weeks. They found that women beyond 40 weeks were more likely to have a failed VBAC (35.4% compared with 26.7%, P < 0.001). ln the adjusted analysis, gestational age more than 40 weeks remained a risk factor for a failed VBAC both for spontaneous (OR 1.5, Cl 1.2 -1.8) and induced labor (OR 1.5, Cl 1.1-2.2). Hammond et al.10 reported their analysis of a cohort of patients attempting VBAC examined by gestational age category. They reviewed records of 329 patients 41 or more weeks of gestation attempting VBAC, comparing those with 2 groups of earlier gestational ages (24-36 6/7 weeks and37-40 6/7 weeks of gestation). They noted a lower rate of VBAC success with advanced gestational age. ln the present study, 147 patients reported in the latent phase and only 6.2 % delivered vaginally, while those who presented in active labor had successful VBAC in 93.8 % patients, a result comparable to findings those of Flamm and Geiger(1997) 11 and Bujold(2004) 7 lt probably indicates, as early as in the latent phase, that the labor might not be a fruitful one. (table A)
Table A: comparison of various studies for cervical dilatation and
Present study shows rate of dehiscence and rupture was 0.76%. Previous studies like Landon et al.12 (0.7%), Lieberman et al. 13 (0.4%) and Wen et al. 14 (0.65%) show similar results. The findings of the present study indicate that the rates of dehiscences and ruptures are well within those acceptable for a trial of vaginal labor following C.S. This also indicates that within the given resources, trial of labor after C.S. is safe and the LUS scar is strong.
CONCLUSION The overall success rate of VBAC trial in this study was comparable to international standards. lnclusion of practice of labor induction in patients with previous one LSCS could have given even better success rates ,though increase in rupture rate and perinatal mortalities also might have increased.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.