 Home
Home
|
Table of Content Volume 13 Issue 3 - March 2020
Cross sectional study on clinico-investigative profile of dengue fever with context to thrombocytopenia
Anil S Mane1, Vaibhav A Padole2*, Chiragkumar K Patel3
1HOD And Professor, 2,3Senior Resident, Department of Medicine, SMBT Institute of Medical Sciences & Research Centre, Dhamangoan, Nashik, Maharashtra, INDIA. Email: vaibhavpadole123@gmail.com
Abstract Background: India is one of the seven identified Southeast Asian countries reporting frequent outbreaks of the dengue with case fatality rates as high as 3-5%. Dengue has an extensive clinical presentation ranging from fever to fatal bleeding and shock, often with an unexpected mortality. Objective: To study clinico-investigative of dengue fever with context to thrombocytopenia. Material and Method: This was descriptive cross sectional study conducted at tertiary care medical teaching hospital of western Maharashtra. Total 200 patients were included in present study as per inclusion and exclusion criteria. Purposive sampling method was used in this study. Structured and pilot tested questionnaire used for data collection. Results. Prevalence of dengue in present study was found to be 4%. Out of 200 patients maximum (53.5%) were in the age group of 15 to 30 years of age and male predominance was seen. In present study out of all patients 97.5% (195) survived where as 2.5% (05) succumbed to dengue. Statistical significant difference was observed in mean hematocrit value of mild and severe thrombocytopenic patients. Most common symptoms observed in current study were headache (77%) and myalgia (76.5%). Mean hospital stay of mild thrombocytopenic patients was 5.92±2.09 days while moderate and severe thrombocytopenic patients mean hospital stay was 6.2±2.74 days and 7.03±3.3 days respectively. Conclusion: The distribution patterns of clinical and laboratory criteria observed did not differ substantially from those described in the literature. Hematocrit and level of thrombocytopenia indicate the prognosis in terms of hospital stay of patients suffering from dengue. Key words: Dengue, Thrombocytopenia, Fever, Hematocrit, Dengue hemorrhagic fever.
INTRODUCTION The fastest spreading vector-borne disease is dengue; which has four serotypes (DEN-1 to DEN-4). There are an estimated 50–100 million dengue fever (DF) worldwide and about 250,000–500,000 cases of dengue hemorrhagic fever (DHF) every year1. In Southeast Asia, the average number of DHF cases per year has increased 10,000 in the 1950s to over 200,000 in the 1990s. Thus, dengue virus has become a major cause of sickness and mortality in tropical areas2. Being a tropical country India has home to variety of infection diseases. India is one of the seven identified Southeast Asian countries reporting frequent outbreaks of the dengue with case fatality rates as high as 3-5%3. Dengue is caused due to female mosquito named Aedes aegypti4. In the year 1956 the first dengue fever in India was reported from Vellore and the first dengue haemorrhagic fever occurred in Calcutta in 19635. In India the annual incidence of dengue is estimated to be 7.5 to 32.5 million6. Dengue is characterized by leucopenia followed by thrombocytopenia. Data from different sources suggest that endothelial cell activation could mediate plasma leakage. Plasma leakage is thought to be associated with functional rather than destructive effects on endothelial cells. Activation of infected monocytes and T-cells, the complement system and the production of mediators, monokines, cytokines, and soluble receptors may also be involved in endothelial cell dysfunction. Hemorrhage may be a consequence of the thrombocytopenia and associated platelet dysfunction or disseminated intravascular coagulation.7All four serotypes of dengue are responsible for severe form like dengue hemorrhagic fever (DHF) and dengue shock syndrome DSS). Dengue has an extensive clinical presentation ranging from fever to fatal bleeding and shock, often with an unexpected mortality. With this background the current study was carried out to determine the clinico-investigative profile of dengue fever in the context of thrombocytopenia.
MATERIAL AND METHOD The permission of the Institutional Ethical Committee (IEC) was sought before commencing the study. This was descriptive cross sectional study conducted at tertiary care medical teaching hospital of western Maharashtra. Informed consent was obtained from the participants and they were assured about the confidentiality of the information. Overall study period for the present study was 02 years. World health organization (WHO) guidelines of classifying and reporting dengue cases were used8. As per guidelines cases were classified as suspected dengue, probable dengue and confirmed dengue. Suspected dengue is a case compatible with the clinical description, which includes: living in or travel to a dengue-endemic area, history of fever, and any two of criteria like nausea, vomiting, rash, aches and pains, leucopoenia, any warning sign. Probable dengue is a case compatible with clinical description and any one of the criteria like positive IgM antibody test in late acute convalescent phase serum specimen or positive Ns1 antigen. Confirmed dengue is case with the clinical description that is confirmed by specific laboratory criteria which includes any one of the criteria like demonstration of a 4 fold or greater change in dengue IgG or IgM antibody titters in paired serum samples or Demonstration of dengue virus antigen or viral genomic sequences from patient samples or isolation of dengue virus from serum, plasma, leucocytes or samples. All the patients who are 15 years and above age, willing to participate, fits as per above guidelines were included in the study. Patients of malaria, typhoid, leptospirosis, or any other dieses causing thrombocytopenia and any preexisting chronic condition that may interfere with assessment of dengue complication were excluded. Total 200 patients were included in present study as per inclusion and exclusion criteria. Purposive sampling method was used in this study. Structured and pilot tested questionnaire used for data collection. Questionnaire consisted of three parts. In Part I; along with socio-demographic information detailed case history regarding history of weakness, vomiting, headache, fever, blurring vision, sleep pattern, duration of fever, abdominal pain etc. were recorded. In part II information on general and clinical examination were recorded. A complete physical examination was carried out. Importance was given to local examination in respect to present condition of patients, any sign and symptoms of disease or any other medical condition involved. Based on the site bleeding score8 was assigned to the patients on daily basis. In Part III data of investigation were recorded. CBC, PCV, SGOT, SGPT, Serum albumin, Dengue IgM, IgG, NS-1, and chest X- ray were carried out for each patients. Using serial haematocrit values and presence of feature indicative of capillary leak or shock, a severity score9 was assigned to the patients. Data was entered into Microsoft Excel and analyzed with SPSS v.16. Descriptive statistics like mean, standard deviation, frequency and proportion were calculated. Inferential statistics like unpaired‘t’ test, chi square test, were used to check association. ‘P’ value <0.05 was taken as statistically significant.
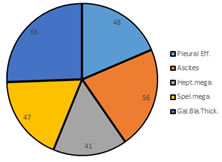
RESULTS In present study total 5000 patients were hospitalized in the tertiary care teaching hospital. Out of 1000 patients 200 tested positive for dengue. All the samples selected for the present study were aged above 15 years of age. Prevalence of dengue in present study was found to be 4%. Out of 200 patients maximum (53.5%) were in the age group of 15 to 30 years of age, 34% (68) and 12.5% (25) were in the age group of 31 to 50 years and above 51 years respectively. The mean age of all participants was 33.77 ± 15 years. Out of 200 patients 118 (59%) were males and 82 (41%) were females. (Graph no 01). Distribution of patients based on severity of dengue shown in table no 01. Out of 200 patients suffering from dengue 68% (137) patient’s hematocrit was less than 40 (Table no 02A). In this study mild thrombocytopenia was seen in 46% (92) cases. (Table no 02B) Most common symptoms observed in current study were headache (77%), myalgia (76.5%), arthralgia (71.5%) and body ache (71%). Nausea/vomiting and retro-orbital pain was less commonly observed. (Table no 03). Out of 200 patients most common complication was ascites (28%) and gall bladder wall thickening (33%) (Graph no 02). Mean SGPT (u/l), mean hemoglobin (g/dl) and mean WBC (cells/mm3) of patients were 32.1±12.68, 13.48±0.5, 3882.52±323.7 respectively. In present study out of all patients 97.5% (195) survived where as 2.5% (05) succumbed to dengue. Mean hematocrit value of patients having mild thrombocytopenia was 37.33±8.1, while moderate and severe thrombocytopenic patients mean hematocrit value were 38.59±8.25 and 40.98±8.35 respectively. Statistical significant difference was observed in mean hematocrit value of mild and severe thrombocytopenic patients on Mann Whitney test. (P=0.03). On comparing the number of patients according to level of thrombocytopenia and severity of dengue, there was no statistically significant difference observed (P= 0.16, table no 04). Average hospital stay of patients was 6.2±2.58 days. Mean hospital stay of mild thrombocytopenic patients was 5.92±2.09 days while moderate and severe thrombocytopenic patients mean hospital stay was 6.2±2.74 days and 7.03±3.3 days respectively. On unpaired‘t’ test statistical significant difference was seen in between mean hospital stay of mild and severe thrombocytopenic patients only (P: 0.03)
DISCUSSION Dengue fever is a common communicable disease and major threat worldwide. It complex nature is a major concern for the clinicians. In present study out all patients 53.5% were between 15 to 30 years of age, 34% and 12.5% were in the age group of 30 to 50 years and above 50 years of age respectively. Mean age of male and females were 35.21±16.29 and 33.90±12.85 years respectively. In this study majority of patients suffering from dengue were males. In Francisca RF et.al.10 study 66 patients were of 15 years old and 88 were of above 15 years age. Vulavala et al.11 in their study reported that majority of the patients were in 18-40 age groups (60.32%) and predominantly were male patients (70.97%). Study conducted by Ahemd S et al.12, Milltal H et al.13, Lee MS et.al14 etc. also reported male predominance in their study. Most common symptoms reported by dengue patients were head ache, body ache and myalgia. In Deshwal R et al.15 study the common symptoms were fever (100%), headache (94.7%), myalgia (90.67%) etc. Lee MS et al.14 in their study found that the most common symptoms of dengue patients were fever (96.1%), myalgia (68.5%), headache (55.4%), and skin rash (53.7%). Ascites, gall bladder thickening and hepatomegaly were common complication seen in present study. Deshwal R et al.15 reported similar finding in his study. Hematocrit value found severely derange in present study and statistical significant difference was observed in hematocrit value of mild and sever thrombocytopenia group. Kittigul L et. al.16 in their study reported hemoconcentration, thrombocytopenia, increased alanine aminotransferase, and longer prothrombin time. Mild thrombocytopenia was seen in 104 patients (52%), moderate in 76 cases (38%) whereas severe thrombocytopenia was seen in 20 cases (10%). In present study severity of dengue was assessed. Of the 200 patients classic dengue fever was seen in 78.5% cases severe dengue 12% cases and dengue hemorrhagic fever was seen in 9.5% cases. With regards to the platelet count mild thrombocytopenia was seen in 52% patients, moderate in 38% patients whereas severe thrombocytopenia was seen in10% patients. On comparing the number of patients according to level of thrombocytopenia and severity of dengue, there was no statistically significant difference observed. Anish Laul et al.17 reported DF in 73%, DHF in 16.5%, DSS in 1.7%, and EDS in 4.3%. In our study the average stay of patients in the hospital was 6.2± 2.58 days. There was a trend of increase in the number of days of hospital stay with regard to the level of thrombocytopenia. In this study 2.5% mortality seen among admitted patients. . Abdul M et al18 in their study reported that mean hospital stay was 10.63 ± 8.434 days in those who died and 1.5% mortality was observed in his study.
CONCLUSION Within the limits of our study we found that males are affected more than females. The distribution patterns of clinical and laboratory criteria observed did not differ substantially from those described in the literature, despite the differences in sample selection criteria between studies. The clinical profile of the patients in our study can be characterized by the presence of fever, headache, bodyache, myalgia, arthralgia, nausea and vomiting. There was an association between the level of thrombocytopenia and the length of hospital stay. The haematocrit levels also corresponded with the level of thrombocytopenia. Thus, haematocrit and level of thrombocytopenia indicate the prognosis in terms of hospital stay of patients suffering from dengue.
TABLES AND GRAPHS Graph 1: Age and gender wise distribution of patients
Table 1: Distribution of patients according to severity (n=200)
Table 2A: Distribution of Hematocrit levels in study participants (n=200)
Table 2B: Distribution of Thrombocytopenia in study participants (n=200)
Table 3: Distribution of clinical symptoms in study participants (n=200)
Graph 4: Distribution of complication of patients
Table 4: Association between severity of dengue and level of thrombocytopenia
REFERENCE
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Community Medicine (Print ISSN: 2579-0862) (Online ISSN: 2636-4743) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.