 Home
Home
|
Table of Content Volume 13 Issue 3 - March 2020
A study of patient characteristics of carpal tunnel syndrome and its correlation with electro-diagnostic findings
Vishali Kotwal1, Amit Thakur2*
{1Associate Professor, Department of Medicine} {2Associate Professor, Department of Orthopaedics} Government Medical College, Jammu, INDIA. Email: thakuramit2277@gmail.com
Abstract Background: Carpal tunnel syndrome (CTS) is one of the most common peripheral neuropathies. It affects mainly middle aged women. In the majority of patients the exact cause and pathogenesis of CTS is unclear. Objective: To study the patient characteristics of CTS and its correlation with electro diagnostic findings. Methods: An observational study was conducted in which 50 patients of carpal tunnel syndrome were taken and after taking a detailed history, physical examination, nerve conduction study was conducted. Boston CTS questionnaire was used to calculate symptom severity scale which included 11 items that assess pain, numbness and weakness at night and during the day. Results: In the current study it was found that females were more than males. Housewives, teachers and office workers were their main occupations. Obesity and hypothyroidism were the two most common comorbidities seen. There was a positive correlation seen with duration of symptoms and electro diagnostic severity however no correlation was seen between clinical symptoms and electro diagnostic severity. Conclusion: CTS is mostly a disease seen in housewives, obese and hypothyroid in our study with no correlation between symptom severity and electro diagnostic severity. Key Words: Carpal Tunnel Syndrome, Obesity, Hypothyroidism, electro diagnostic severity
INTRODUCTION Carpal Tunnel Syndrome is a clinical disorder resulting from compression of Median Nerve inside the carpal tunnel at wrist. It is the most common entrapment neuropathy with an estimated prevalence of 2-3%1,5.8% in women and 0.6% in men 2 and a lifetime risk of 10% with an unadjusted incidence in adults of 1 per 1000 person-years.3 It is seen 3 times more often in women than in men. It is most commonly observed in women between the ages of 40 and 60 years. So, Carpal Tunnel Syndrome is a significant public health problem and is associated with substantial disability. The symptoms of Carpal Tunnel Syndrome range from pins and needles sensation and numbness in the distribution of the median nerve to pain which is aggravated mostly during night-time.4 Sensory symptoms are also felt in areas other than Median nerve and whole hand is affected.5 Pain and paraesthesia are sometimes felt in forearm and shoulder due to central sensitization.6,7 In advanced stages, there is atrophy of the thenar eminence of hand with weakness in muscles supplied by median nerve. The exact cause and pathogenesis of Carpal Tunnel Syndrome is not known and various risk factors include diabetes mellitus, hypothyroidism, obesity, Rheumatoid arthritis, pregnancy, trauma or tumours like ganglion, lipoma and xanthoma. It is also seen to be associated with occupations involving hand and wrist exposure to a high pressure or repetitive work and vibrating tools.8,9,10 The diagnosis of Carpal Tunnel Syndrome can be made from history, physical examination which includes provocative tests i.e. Tinel's and Phalen's sign 11,12 and electro diagnostic findings on nerve conduction study.13 The present study was carried out to study the various patient characteristics of carpal tunnel syndrome and to study the relationship between electro diagnostic findings and patient symptoms in Carpal Tunnel Syndrome. Aim: To study the patient characteristics of CTS and its correlation with electro diagnostic findings.
MATERIAL AND METHODS The present study was carried out at the Department of Medicine GMC Jammu with effect from June 2017 to Jan 2018. It was an observational study in which 50 cases of carpal tunnel syndrome who more than 18 years of age were enrolled and evaluated. Patients with a history of trauma to hand, a hand or wrist surgery in the past 1 year, patients with mass, tumour or deformity or fracture of hand or arm were not included in the study and also the patients with polyneuropathy and cervical radiculopathy were excluded. A detailed history including age, symptom duration, occupational history, personal history including smoking history, history of medical comorbidities like diabetes, hypothyroidism, rheumatoid arthritis etc. was taken. Also a detailed physical examination was done which included BMI, complete neurological examination of both the hands. Boston CTS questionnaire was used to calculate symptom severity scale which included 11 items that assess pain, numbness and weakness at night and during the day. Each question is answered on a 1-5 scale with higher scores indicating greater severity. The BCTSAQ has established responsiveness, validity and reliability
Routine tests were done which included Blood sugar (Fasting), Thyroid function tests, ESR, RA factor, Lipid profile, RFT's, LFT's. Nerve conduction test was done on both hands. NCS was done on Recorders and Medicare Systems Machine. Motor nerve conduction was done by using surface electrodes placed over Abductor Pollicis Brevis for median nerve and Abductor Digiti minimi for Ulnar nerve and stimulating 3cm proximal to the distal crease of wrist. Sensory nerve conduction was done by antidromic stimulation using ring electrodes for recording placed over index finger in case of Median nerve and ring finger in case of Ulnar nerve and stimulating over mid-palm and wrist. CTS was diagnosed if any one of the following electro diagnostic findings were present.
Carpal tunnel syndrome was classified as mild, moderate and severe groups according to nerve conduction findings. Mild CTS was diagnosed if NCS showed a prolonged distal motor latency but less than 5.4ms or a slowed SNCV but greater than 30.1meters per second or reduced CMAP or SNAP but greater than 3.9millivolts and 6.1microvolts respectively. Moderate CTS was diagnosed if distal motor latency was between 5.2 -7.2 milliseconds or SNCV was 20-30 meters per second or CMAP or SNAP was 2.5-3.8millivolt and 4-6 microvolt respectively. Severe CTS shower either distal motor latency over 7.2milliseconds or SNCV less than 20 meters per second or not obtainable or CMAP or SNAP below 2.5 millivolt or 4 microvolt respectively Abnormal result in any one of the three categories, including a prominently prolonged distal motor latency, a markedly slowed SNCV, a reduced amplitude of CMAP or SNAP is enough to diagnose a case as mild, moderate or severe. Statistical Analysis: The collected data was evaluated using Mean, Percentages and Correlation; SPSS software was used.
RESULTS A total of 50 patients (100 hands) were studied out of which CTS was diagnosed in 86 hands. Median age of the patients was 49.5 years with range from 20 to 75 years.37 (74%) were females and 13 (26%) were males. Only 5 patients were left handed.19 patients had symptoms for less than 6 months, 26 between 7to 11months and only 5 patients had symptoms for 12 or more than 12 months. Hypothyroidism was present in 27 patients as a comorbid condition,9 patients were diabetic, obesity was present in 28 patients and rheumatoid arthritis was seen in 4 patients. 23 females were housewives, 9 patients were teachers by occupation, 8 were working in an office, 3 were computer operators, 2 were students and 3 were manual workers. Clinical severity score (BCTSAQ) was mild in 13, moderate in 13 and severe in 24 patients. (Table 1)
Table 1: Showing Clinical Characteristics of Patients
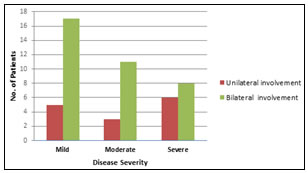
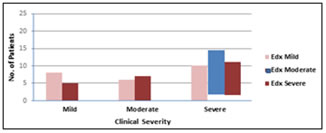
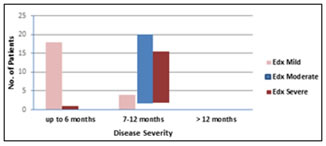
Bilateral disease was seen to be present electro diagnostically in 36 patients while 14 patients had unilateral disease. Right side was more involved than left in 19 patients, while left was more involved than right in 4 patients and 13 patients had equal severity on both sides. Pure sensory involvement was seen in 9 patients. Electro diagnostic severity was mild in 22 patients, moderate in 14 patients and severe in 14 patients. There were 2 cases of concomitant ulnar nerve compression. (Table 2; Figure 1,2,3) Table 2: Showing Electrodiagnostic Features Of Patients
Figure 1: showing distribution of unilateral or bilateral disease according to disease severity Figure 2: showing correlation between clinical and electro diagnostic severity Figure 3: showing Correlation Between Duration Of Symptoms And Electrodiagnostic Severity
DISCUSSION In our study, out of 50 patients (100 hands), 86 hands were having CTS. Female cases were more as compared to males (Female:Male ratio was 3:1) Maximum patients were in the age group of 40 to 60 years. These findings are consistent with those of Goyal et al.14 Most of the patients were housewives . Obesity and hypothyroidism were the most common comorbidities seen in more than half of the patients similar to the study by Kasundra GM et al.15 Most common symptom was paraesthesia present in 80% of the patients. Most of the patients had symptoms for less than 1 year which shows that symptoms start early in the course of the disease. Disease duration showed a correlation with electro diagnostic severity similar to the study by Tay LB et al.16 Bilateral disease was more as compared to unilateral disease and even patients with unilateral symptoms were seen to have involvement of the other side as well on nerve conduction study.Dominant hand was involved in most of the cases. Malibary et al.17 also found bilateral involvement more as compared to unilateral involvement. Clinically, more patients were having severe symptoms (48%) than detected by electrodiagnosis(24%) and electrodiagnostic severity did not correlate with clinical severity. This has also been observed in some previous studies. Leighton Chan et al.18 in their study found that there was no statistically significant relationship between electro diagnostic findings and the patient functional status and symptom severity. Firosh Khan et al.19 also found in their study that subjective symptoms of CTS correlated more with psychological factors than with electrophysiological severity.Itsubo et al.,20 Longstaff et al.,21 De Campos et al.,22de la Llave et al.23,Schrijver H M et al.24, and Makanji et al.25 found similar results in their studies. Simultaneous involvement of the ulnar nerve was seen in 2 patients. The cause for discrepancy in patient related symptoms and electro diagnostic findings may be due to differential involvement of thin myelinated A delta and unmyelinated C fibres early in the course of the disease which carry the pain sensations and their dysfunction is not picked up in nerve conduction studies. Thick myelinated A Beta fibres are involved at a later stage and their involvement results in the electro diagnostic findings in nerve conduction studies.26 Another reason may be that patient is not used to the new onset symptoms early in the course of the disease but later on he is habituated and compensated, so has less symptoms. Moreover, painful symptoms of CTS are also dependent on the psychological state and mood of the patient 27 which should also be evaluated.
CONCLUSION In our study, CTS is seen to be more in females, obese and hypothyroid patients with bilateral involvement in most of the cases. Majority of the patients had symptoms for the last less than 1 year. Severity of the disease correlated with the duration of symptoms while clinical severity had no correlation with electro diagnostic severity. So, symptoms alone cannot be considered in determining the severity of CTS and its definitive treatment but electro diagnostic studies should be considered together and also psychological status of the patient should be evaluated and further studies are needed to see this correlation with mood of the patient.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Community Medicine (Print ISSN: 2579-0862) (Online ISSN: 2636-4743) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.