 Home
Home
|
Table of Content Volume 14 Issue 2 - May 2020
Anil S Mane1, Chiragkumar K Patel2*, Vaibhav A Padole3
1HOD And Professor, 2,3Senior Resident, Department of Medicine, SMBT Institute of Medical Sciences & Research Centre, Dhamangoan, Nashik, Maharashtra, INDIA. Email: chirapatelhospital@gmail.com
Abstract Background: Rapid epidemiological transition in India with increased urbanization and westernization has contributed substantial rise in diabetes. Diabetes mellitus (DM) is a heterogeneous group of disease, characterized by a state of chronic hyperglycemia resulting from a diversity of etiologies, environment and genetic action jointly. These diversities of DM, mandate us to study its clinical and investigative profile. Objective. To study clinic-investigative profiles of newly diagnosed type II diabetes patients. Material and Methods: Newly diagnosed 100 type II diabetes patients were studied in present cross sectional study. Simple random sampling method used to select the participants. Results: Out of 100 majority of patients were in the age group of 51-60 years and gender distribution found to be somewhat similar. Most common symptoms were found to be polyuria (24%) followed by tingling and numbness (18%). Fasting and post prandial sugar and HBA1C level found to be statistical significant among diabetic microvascular and non microvascular complication groups. Conclusion: Adults should be screen earliest to diagnose diabetes and to prevent its complications. Keywords: Diabetes mellitus, type II, Polyuria, Tingling, Numbness.
INTRODUCTION Diabetes mellitus is heterogeneous metabolic disorder that arises due to a decrease in insulin secretion or when the body is unable to use insulin effectively. Insulin is a hormone required to regulate blood sugar or glucose1 and absence of this function leads to a chronic hyperglycemic state. The estimated global prevalence of diabetes is 387 million (8.3%) and is projected to increase to 592 million by 2035 (IDF).2 India is the diabetes capital of the world with 41 million Indians having diabetes; every fifth diabetic in the world is an Indian.3 Rapid epidemiological transition in India with increased urbanization and westernization has contributed substantial rise in diabetes.4 In India urban and rural prevalence of diabetes ranges from 5.6% to 12.4% and 2.4% to 2.7% respectively.5 Undiagnosed and inadequate treatment of diabetes may result into multiple complication which may lead to irreversible disabilities and deaths. Age, positive family history, obesity, hypertension, sedentary lifestyle, socioeconomic class etc. are known risk factors for diabetes mellitus. So far a lot of research has been done on diabetes mellitus but still not much is known about it; it is complex etiopathogenesis, generating eagerness among researchers to study it continuously.
MATERIAL AND METHODS Institutional ethical committee’s permission (IEC) was obtained before commencement of study. This was cross sectional study conducted on out patients (OPD) of medicine department. Present study was conducted for the period of two years. All the newly diagnosed diabetes mellitus patients of either gender, who are willing to give informed consent were included in this study. Patients who are either less than 30 years or more than 70 years, having history of chronic diseases like cancer, kidney diseases etc. were excluded. Total 100 patients were recruited by using simple random sampling method. Structured and pilot test questionnaire was used for data collection. Questionnaire consisted of three parts. Part I included information on socio-demographic status, symptoms suggestive of diabetes mellitus and its complication. In part II family history of diabetes mellitus, history of hypertension, ischemic heart disease, stroke, addiction, physical activity were documented. In part III information on general and clinical examination were recorded. In general examination pulse, blood pressure, temperature, respiratory rate along information on anthropometric variable viz. height, weight, body mass index, waist circumference were recorded as per standard protocol. In clinical examination signs of skin infection, gangrene, ulcer, sensory neuropathy, motor neuropathy, and autonomic dysfunction were recorded. To detect proliferative and non-proliferative retinopathy dilated fundoscopy were carried out in all patients with the help of ophthalmologist. Data was entered into Microsoft Excel and analyzed with SPSS v.16. Descriptive statistics like mean, standard deviation, frequency and proportion were calculated. Inferential statistics like ‘t’ test, Pearson’s correlation were used to check association. ‘P’ value <0.05 was taken as statistically significant.
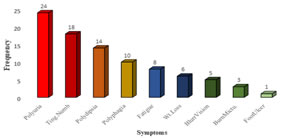
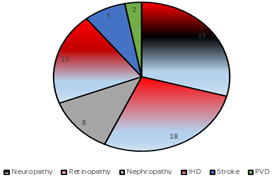
RESULTS In present study total 100 newly diagnosed patients of diabetes mellitus were studied. Out of that 54% were males and heart 46% were females. The mean age of the patients was 51.64 ± 9.51 years. Majority of diabetes patients were of 51-60 years (33%) of age. other common involved age groups were 41 to 50 years and 61 to 70 years. In present study most frequent symptoms were polyuria (24%), tingling numbness (18%) and polydipsia (14%) etc. (graph no 01). In present study 19% and 18% patients had diabetic neuropathy and diabetic retinopathy respectively. Other complication were ischaemic disease (13%), diabetic nephropathy (8%), cerebrovascular stroke (5%) and peripheral vascular disease (2%). (Graph no 02) Out of total patients 52% had normal BMI, 44% and 04 % patients were overweight and underweight respectively. The mean BMI of the patients was 25.02 ± 3.33. Out of 56 males 21.42%% males had high waist hip ratio (WHR>01) while out of 44 females 54.54% had high waist hip ratio (WHR>0.85). The average waist hip ratio of all participants was 0.89 ±0.09. Positive family history of diabetes mellitus was seen in 20% male and 15% female patients. Clinico-investigative profile of all patients shown in table no 01. Mean fasting blood sugar (FBS) levels among patients having diabetic retinopathy and not having retinopathy were 358.44±43.07 and 239.09±85.64 respectively. Among diabetic nephropathy and non-nephropathy patients mean fasting blood sugar level was 352.75±47.44 and 252.55±90.55 respectively. Patients of having diabetic neuropathy also has higher mean fasting blood sugar level (343.85±75.0) than non-diabetic neuropathy patients. In all there group’s statistical significant difference was seen in fasting sugar level. (Table no 02) Among diabetic nephropathy and non-nephropathy patients mean post prandial blood sugar (PPBS) level was 475.13±45.30 and 278.63±61.79 respectively. Mean post prandial blood sugar level was higher in patients having diabetic retinopathy (365.11±63.02) than non-retinopathy (278.81±76.06) patients. In diabetic neuropathy patients mean post prandial blood sugar level was 337.30±60.34 while in non-diabetic neuropathy patients it was 283.61±81.96. PPBS levels were found to be statistical significant among patients having diabetic complication and not having complication. (Table no 03) Mean HbA1C level among patients having and not having diabetic retinopathy was 10.52 ± 1.77 and 8.67 ± 1.53 respectively. Among diabetic nephropathy patients mean HbA1C level found to be higher (10.84±1.79) than not having nephropathy (08.84±1.63). In diabetic neuropathy patients mean HbA1C level was 10.41±2.04 and not having neuropathy it was 08.65±1.45. The difference of mean HbA1C level found to be statistical significant. (Table no 04) Among patients having tingling numbness and not having numbness; difference among FBS level, PPBS level and HbA1C level found to be non-significant (Table no 05). Patients having blurring of vision and not having blurring of vision; difference of FBS level and PPBS level found to be statistically significant while difference of HbA1C level found to be not significant. (Table no 06). Pearson’s correlation test between HbA1C level and lipid profile found to be not significant. (Table no 07)
DISCUSSION Present cross sectional study conducted on hundred newly diagnosed diabetes mellitus patients attending out patients department of medicine. Out of all 54% were males and 46% were females, ratio of male to female was 1.17: 1 and majority of diabetes patients were of 51-60 years (33%) of age. Study conducted by Cassamo PA et al.6 also reported 50 to 60 years as common age group. In his study male to female ratio was 0.78:1. In our study according to BMI, 52% patients were having normal weight while 44% were overweight and 4% were underweight. According to WHR criteria, 36% of all study subjects were obese (Male 12 and Female 24). Mean BMI of the patients was 25.02 ± 3.33. Study done by Cassamo PA et al on type 2 diabetes mellitus patients reported mean BMI level of 31.9 and 90% were obese. These findings are significantly higher than current study findings. In present study, mean levels of FBS, PPBS and HbA1C were 266.77, 294.34 and 9.00, respectively. Study done in Cassamo PA et al6 reported increased blood sugar in 22.34% and increased HbA1C in 36.67% of study participants. In our study positive family history of diabetes mellitus was seen in 20% male and 15% female patients. Kumar R et al.7 reported positive family history in 36.2l% of female and 47.86% of males. In present study, most common symptom was Polyuria (24%) followed by tingling and numbness (18%), polydip0sia (14%) and polyphagia (10%). Other symptoms were fatigue, weight loss, blurring of vision, burning micturition and foot ulcer. Kumar R et.al7 reported polyuria as most common symptoms (30%) followed by tingling numbness (26%), blurred vision (26%), polyphagia (24%), altered sleep (24%), weakness (22%) and other symptoms like decreased appetite, burning micturition, skin manifestation and chest pain. Similar findings were noted in present studyIn present study 19% and 18% patients had diabetic neuropathy and diabetic retinopathy respectively McDowell D et al.8 reported 28.5% prevalence of neuropathy. They also found that there was no difference in the prevalence of neuropathy between males and females. In a study conducted by Kumar R et al.7 retinopathy was present in 28% of the patients being significantly higher in males (32.5%) than in females (20.3%). In same study coronary artery disease and peripheral vascular disease (PVD) were present in 14 % and 17 % of subjects respectively being -more common in males. In present study, no significant correlations were found between various lipid profile parameters and HbA1C levels. Study done by Chowdhury TA et al9 revealed that serum total cholesterol, LDL cholesterol and triglycerides were significantly raised whereas the level of HDL cholesterol was significantly lower in diabetic subjects
CONCLUSION Present study concluded that male and female have somewhat similar predisposition for diabetes mellitus. Commonest symptoms among diabetes are polyuria, polydipsia and polyphagia etc. Diabetic neuropathy and nephropathy are commonest complication among study participants and adults should be screen earliest to diagnose diabetes and to prevent its complications.
TABLES AND GRAPHS Graph 1: Distribution of symptoms Graph 2: Distribution of complication
Table 1: Clico-investigative profile of diabetes mellitus patients (n=100)
Table 2: Mean FBS# among diabetic retinopathy, nephropathy and neuropathy
#:FBS: Fasting blood sugar level, *:Significant
Table 3: Mean PPBS# among diabetic retinopathy, nephropathy and neuropathy
#PPBS: Post prandial blood sugar level. *: Significant
Table 4: Mean HbA1C among diabetic retinopathy, nephropathy and neuropathy
*: Significant
Table 5: FBS, PPBS and HbA1C among tingling numbness and not having tingling numbness
Table 6: FBS, PPBS and HbA1C among tingling numbness and not having tingling numbness
Table 7: Pearson’s Correlation in between HbA1C and Lipid Profile
REFERENCE
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Community Medicine (Print ISSN: 2579-0862) (Online ISSN: 2636-4743) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.