 Home
Home
|
Table of Content Volume 14 Issue 2 - May 2020
A study of clinical profile of the patients with acute hepatic encephalopathy in a tertiary health care centre
Manjiri Ravindra Kulkarni
Associate Professor, Department of Medicine, R. K. D. F. Medical College Hospital & Research Centre, Bhopal (M. P.), Jatkhedi, Nh-12, Hosingabad Road, Bhopal, Madhya Pradesh, INDIA.
Abstract Background: liver cirrhosis is one of the debilitating conditions in liver diseases. Acute hepatic encephalopathy is affecting neurological and psychiatric conditions of the patients with liver disease. Hepatic encephalopathy can be reversible with treatment reducing the mortality rate. Aim and objective: To study the clinical of the patients with acute hepatic encephalopathy in a tertiary health care centre Methodology: An observational study was done on 100 patients with Acute hepatic Encephalopathy. Data collected with pre tested questionnaire. Sociodemographic data, clinical history and detailed clinical examination was done. All required investigations carried out. Patients were followed upto discharge from hospital. Clinical features, precipitating factors and outcome was analysed with appropriate statistical tests. Results and discussion: Mean age of the patient was 38 ± 2 years. Male to female ratio was 2.7:1. Jaundice,ascites, anaemia, upper GI bleed and splenomegaly were common clinical features in all patients. Common precipitating factors were Upper GI bleed (30%), fever indicating infection (42%) and constipation (35%). In our study alcoholic liver disease was most common etiological factor (43%). Hepatitis B infection was seen in 33% and Hepatitis C infection in 12% patients. Factors affecting mortality in hepatic encephalopathy were Male sex, alcohol intake, Child-Pugh Class C, Grade III and IV hepatic encephalothy and infections like Hepatitis B and Hepatitis C. Key Word: acute hepatic encephalopathy.
INTRODUCTION Hepatic encephalopathy is a brain dysfunction caused by liver impairment which manifests as a wide spectrum of neurological or psychiatric abnormalities. 1 It is a dreadful complication of cirrhosis. The risk for the first episode of hepatic encephalopathy is 5–25% within 5 years after the diagnosis of cirrhosis and is greatest in those with decompensated liver disease.2Acute hepatic encephalopathy may be precipitated by a number of diverse events, such as infection, gastrointestinal haemorrhage, electrolyte disturbance, alcohol misuse or constipation, although in 50% of instances no obvious cause is identified.3 These acute precipitating events can be infectious or non-infectious. There is a difference between the western countries and the eastern countries in the major etiological agents. Viral infections are more common in the east whereas alcohol and drugs are more common in the west 4-6 Among infectious causes reactivation hepatitis B virus infection is one of the major cause. Various bacterial, spirochetal and fungal infections can also affect the liver. Among the noninfectious causes alcoholic hepatitis is a common cause. Other causes include drug induced liver injury and surgery. Acute hepatic encephalopathy is reversible with treatment. The reversibility depends on the severity and nature of acute insult and degree of underlying chronic liver disease. So Present study was conducted to study the clinical profile of the patients with acute hepatic encephalopathy in a tertiary health care centre.
Aim and Objective: To study the clinical of the patients with acute hepatic encephalopathy in a tertiary health care centre Methodology: Present study is an observational study carried on patients with acute hepatic encephalopathy patients attending OPD and emergency in surgery department of a tertiary health care centre. Inclusion criteria: 1. Patients with signs and symptoms of acute hepatic encephalopathy (Gastrointestinal bleeding like Haematesis or malena, fever, vomittimg, diarrhoea, constipation etc)2. Patients above age of 18 years Exclusion criteria: 1. Patients below 18 years 2. Patients with acute alcohol intoxication and alcohol withdrawal state 3. Patients with liver maliganancies 4. Patients with neurological and psychiatric diseases. Study was approved by ethical committee. A valid written consent was taken from the patients after explaining study to them. Total 100 patients with inclusion criteria were studied. Data was collected with pre tested questionnaire. Data included sociodemographic data like age, sex. Detailed history was taken from the patients. Medicine history like sedatives, NSAID and diuretics was taken. Through clinical examination was done by principal investigator. All Patients underwent investigations like CBC, Liver function tests, renal function tests, serum electrolytes, HBs Ag And Anti HCV, Xray chest, abdomen Ultrasound. According to progress of patients other investigations like upper GI scopy, serum ceruloplasmin, 24 hr urinary copper excretion, serum ferritin, transferrin saturation was done if required. Hepatic encephalopathy was graded according to West Haven classification (Table A) and severity of liver cirrhosis was done with Child-Pugh score system (Table B). Child Pugh score system has three grades. Grade A(5-6 points) , B(7-9 points) and C(10-15 points). All patients were given symptomatic treatment. Specific treatment was given according to progression of disease. All patients followed until their stay in hospital. Outcome was analysed as death or discharge of patients. Data was analysed with appropriate statistical tests.
Table A:Clinical Grades of Hepatic Encephalopathy West Haven classification
Table B: Child-Pugh Score
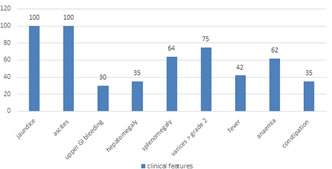
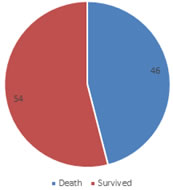
RESULTS Total 100 patients were studied. Mean age of the patient was 38 ± 2 years. Table 1 shows distribution of patients according to age. Majority of the patients were in the age group of 41- 50 years (36%) followed by 31-40 years (23%). Patients were less in the age group below 20 years (3%) and above 60 years (6%). Out of total 100 patients 73 were male and 27 were females. Male to female ratio was 2.7:1. Figure 1 shows clinical features among the patients. Jaundice and ascites were common clinical features in all patients. Anaemia was seen in 62% patients. Upper gastrointestinal bleed was seen in 30 % patients. Splenomegaly and hepatomegaly were seen in 64% and 35% patients respectively. Fever was observed in 42% patients. Constipation was observed in 35% patients. Common precipitating factors were Upper GI bleed (30%), fever indicating infection (42%) and constipation (35%). Among the patients with infection most commonly recorded was spontaneous Bacterial Peritonitis (SBP)(53%) followed by urinary tract infection (33%) and pneumonia and septicaemia (14%). In our study alcoholic liver disease was most common etiological factor (43%). Hepatitis B infection was seen in 33% and Hepatitis C infection in 12% patients. Six patients showed alcoholic liver disease with hepatitis B infection. Unknown etiology was observed in 6% patients. According to Child Pugh score, 58 % patients were in group A followed by Group B (34%) and Group C (8%). Table 4 showed distribution of patients according to West Haven classification. Majority of the patients were in Grade IV (36%), followed by Grade III (32%). Grade I included 20% patients and Grade II included 12%. Our study revealed majority patients were of type C (82%) Hepatic encephalopathy followed by type A (18%). All patients were followed up to discharge from hospital. Out of 100 patients 54 patients survived and 46 patients died. According to Child Pugh Score patients with Group A had 100% survival. Group B has 27% mortality and Group C has highest mortality of 73%. In our study we found that Grade I of West Haven classification has zero mortality. Mortality increases as the grade increases in the patients (Grade II : 28%, Grade III : 38% and Grade IV : 94%). All parameters like haemoglobin, serum Na, serum K and Liver enzymes were elevated in all patients. Parameters were elevated in patients who died as compared to those who survived.
Table 1: Distribution of patients according to age group
Figure 1: Distribution of patients according to clinical features
Table 2: Distribution of patients according to etiology
Table 3: Distribution of patients according to Child Pugh Score
Table 4: Distribution of patients according to West Haven classification
Table 5: Distribution of patients according to Type of hepatic encephalopathy
Figure 2: Distribution of patients according to outcome
DISCUSSION Mean age of the patient was 38 ± 2 years. Similar findings were seen in Onyekwere CA et al..7Majority of the patients were in the age group of 41- 50 years (36%) followed by 31-40 years (23%). Similar findings were seen in Saira Afzal et al. 8(64%), Alam et al. 9(64%). Most commonly affected population was 41-60 years in a study by Bikham Devrajani et al.10. In our study Male to female ratio was 2.7:1. Similar findings were seen in various studies like Dhiman RK et al. 11and Shivani Patel et al. where male preponderance was seen. Jaundice and ascites were common clinical features in all patients. Anaemia was seen in 62% patients. Upper gastrointestinal bleed was seen in 30 % patients. Splenomegaly and hepatomegaly were seen in 64% and 35% patients respectively. Similarily jaundice and ascites were found as commonest features in patients in studies like Alam et al.9 and Khurram et al..12 Anaemia was seen in 85% of cases by Jadumani Nayak et al..13 In our study alcoholic liver disease was most common etiological factor (43%). It is in accordance with study by Medha Rao et al. where 58.1% patients showed alcohol associated cirrhosis. Hepatitis B infection was seen in 33% and Hepatitis C infection in 12% patients. In a study by Sarin SK et al.14 HBV was common prevalent factor for hepatic encephalopathy. Study by Mumtaz et al. 15 showed Anti HCV was positive in 70% patients. Hepatitis C virus was the commonest of Cirrhosis by Muhammad Khurram et al..12Unknown etiology was observed in 6% patients. In a study by Ashish et al.16 cryptogenic causes were 35% in chronic liver diseases. According to Child Pugh score, 58 % patients were in group A followed by Group B (34%) and Group C (8%). Majority of the patients were in Grade IV (36%), followed by Grade III (32%). Grade I included 20% patients and Grade II included 12%.Our study revealed majority patients were of type C (82%) Hepatic encephalopathy followed by type A (18%). Out of 100 patients 54 patients survived and 46 patients died. Similar findings were seen in study by Onyekwere CA et al.7(51%). According to Child Pugh Score patients with Group A had 100% survival. Group B has 27% mortality and Group C has highest mortality of 73%. In accordance with our study higher mortality was seen in Group C by Fakhar Ali Qazi Arisar et al.17 In our study we found that Grade I of West Haven classification has zero mortality. Mortality increases as the grade increases in the patients (Grade II : 28%, Grade III : 38% and Grade IV : 94%). Similar findings were seen in Alam et al. 9and Bikha Ram Devrajani et al. 10.
CONCLUSION Factors affecting mortality in hepatic encephalopathy were Male sex, alcohol intake, Child-Pugh Class C, Grade III and IV hepatic encephalopathy HBsAg, HCV antibody, low haemoglobin and elevated liver and renal parameters
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Community Medicine (Print ISSN: 2579-0862) (Online ISSN: 2636-4743) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.