 Home
Home
|
Table of Content Volume 14 Issue 2 - May 2020
A study of cardiovascular risk factors profile in young patients with acute myocardial infarction
Sapkal Harish Barsu1, Chandrakant Raibhoge2*, Deshpande Neelima S3, Dawle Kiran4
1Assistant Professor, Department of Medicine, Government Medical College, Nagpur, Maharashtra, INDIA. 2Associate Professor, 3Professor & HOD, 4Assistant Professor, Department of Medicine, Government Medical College, Latur, Maharashtra, INDIA. Email: harishsapkal2012@gmail.com
Abstract Background: MI in young patients carries a significant morbidity, psychological effects and financial constraints for the person and the family. Aim and objective: To study the cardiovascular risk factors profile in young patients with acute myocardial infarction Methodology: Present study is an observational Descriptive study of clinical profile of patients admitted with a diagnosis of acute MI during the study period 2 years.50 patients fulfilled the inclusion criteria during the study period. Data collection included sociodemographic data, clinical history, investigations for diagnosing MI. Data analysed with appropriate statistical tests. Results and discussion: out of total patients 88 % presented with typical chest pain and 12 % presented with atypical symptoms. 48 % had anterior wall MI and 38% had inferior wall MI. Cardiac biomarker, CKMB was elevated in 90% and TROP T in 94%. Smoking was the most common risk factor contributing to 68%, followed by dyslipidemia at 64%, metabolic syndrome contributed to 38%, diabetes to 26%, hypertension to 28%, positive family history to 18% and chronic kidney disease to 4%.
INTRODUCTION Cardiovascular diseases are one of the major health problems reaching epidemic proportions. In fact they are the most common cause of deaths in the world followed by cancer. Previous studies have reported that there is a rising incidence of acute myocardial infarction in the young. Although acute MI is an uncommon entity in the young, it constitutes the incidence is increasing in young patients and has become important problem for such patients and their treating physicians because of its devastating effect on their more active lifestyle. Hence it is important to identify and control cardiovascular risk factors at an early age to prevent the incidence in cases of young MI, to reduce the risk of MI at young age, to reduce the severity and complications. So this study was carried out clinical profile, risk factors, complications and outcome in these young patients. There is a rising incidence of acute MI in young adults.1Although acute MI mainly occurs in older patients, young men and women can suffer MI. This disease carries a significant morbidity, psychological effects and financial constraints for the person and the family when it occurs at a younger age.2 The causes of MI among patients in younger age group can be divided into four groups, 1. Atheromatous coronary artery disease. 2. Nonatheromatous coronary artery disease. 3. Hypercoagulable states 4.MI related to substance abuse. A majority of young adults with acute MI have at least one identifiable risk factor.3 The risk factors noted are smoking, diet rich in cholesterol, sedentary lifestyle, diabetes, hypertension, paternal history of cardiovascular disease.4 The pathophysiology of MI in the presence of normal coronary arteries can be explained on the basis of coronary artery thrombosis, embolization, spasm, or a combination of these processes. Coronary thrombosis can be seen in hypercoagulable states such as in the nephrotic syndrome, antiphospholipid syndrome, and protein C and S and factor XII deficiencies.5 Young patients with acute MI may be characterized by two distinctive patterns; One associated with smoking and a higher physical activity level at the onset of acute MI with a 0-1 vessel disease and the other with hypertension and hypercholesterolemia with a multivessel disease.6 In India the incidence of premature coronary heart disease is 12-16%.7 About 25% of acute MI in India occurs under the age group of 40 and 50% under the age group of 50. One center reported a 47 fold increase in the incidence of first MI under the age of 40 in the last 20 yrs.8 Younger patients also featured a higher incidence of single vessel and a lower rate of triple vessel disease. In those with MI secondary to accelerated premature atherosclerosis, early intervention with primary angioplasty has an improved outcome over thrombolysis.9 we can prevent the disease by knowing in detail about risk factors so this study was conducted to study the cardiovascular risk factors in young patients with acute myocardial infarction. Aim and objective: To study the cardiovascular risk factors profile in young patients with acute myocardial infarction
MATERIAL AND METHODS Present study is a descriptive observational study carried out in Department of Medicine at a Tertiary care centre. Patients aged 40 years or younger admitted to with a diagnosis of acute MI in a tertiary care centre in Maharashtra during the period of the study (2017-2018) were included in the study. Inclusion Criteria: 1.All patients aged 40 years or younger admitted. Exclusion Criteria: 1.Patients aged < 18 years 2.Those patients 40 years or younger with acute MI who refused to give their written informed consent for the study. The final diagnosis of acute MI will be based on two of the following criteria : 1.Ischemic chest pain for at least 30 minutes. 2. ECG evidence of myocardial injury (0.1 mv or more ST segment elevation in 2 contiguous leads or 0.1mv or more ST depression or definite T-wave inversion or both. An increase in serial CKMB or serial troponin). There were 50 patients who participated in the study. Study was approved by ethical committee of the institute. A valid written consent was taken from patients after explaining study to them.Data was collected with pretested questionnaire. Data included sociodemographic data, clinical history of the patients. A through clinical examination was done. Diagnostic evaluation was done. Cardiovascular risk factors were noted. The weight and height measurements were converted into body mass indexBMI=weight(kg)/(Height meteres)2 Statistical analysis will be carried out with the help of SPSS (version 20) for Windows package (SPSS Science, Chicago, IL, USA). The description of the data will be done in form of arithmetic mean +/- SD for quantitative data while in the form of frequencies (%) for qualitative (categorical) data. P-values of< 0.05 will be considered significant. For comparison of categorical variables (i.e. to examine the associations between qualitative/quantitative variables), chi-square test will be used if the number of elements in each cell are 5 or higher and Fisher’s exact test, otherwise. To compare proportions between two independent groups Z test of proportions will be used. Risk factor analysis was done using odds ratios (OR) along with their respective 95% confidence intervals (CI) for finding risk factors of under-nutrition.
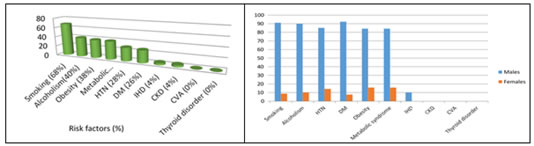
RESULTS In present study we recruited 50 patients. In this study, majorities were males (88%), and only 6 patients (12%) were females.(table1) Patients belonged to age groups varying from 20 yrs to 40 yrs with a mean age of 34.16±4.81. Majority of patients belonged to age group of 36-40 yrs 28 (56%). (table2) It was found that a majority of patients had an increased BMI. There were 14 patients out of the total 50 had a normal BMI (28%). 28 patients had BMI between 25-30 kg/m2(56%). 8 patients had BMI between 31-35 kg/m2(16%). (table3) Majority of patients presented with typical chest pain. 5 patients presented with atypical symptoms, one had only sweating, two had heaviness of chest, one had epigastric pain, one had sudden collapse. On ECG, 24 patients had AWMI (48%), 3 had anterolateral, 1 had anterior and inferior wall MI and 2 had anteroseptal MI. A total 38% i.e. 21 patients had inferior wall MI (IWMI- 42%) Out of 50 patients, 68% patients have smoking addiction. Family H/O out of 50 patients with MI, 2% have IHD, 24% have DM, and 36% have HTN. Out of 50 patients, 47 (94%) patients have increased Trop I and 3(6%) patients have normal Trop I. Out of 50 patients, 45 (90%) patients have increased serial CPK MB and 5(10%) patients have normal serial CPK MB.(table 4) Among 50 patients studied, 36 (72%) had increased total cholesterol, 46 (92%) had increased TG, 5 (10%) had increased LDL and 6 (12%) had decreased HDL levels. On ECG, 24 patients had AWMI (48%), 3 had anterolateral, 1 had anterior and inferior wall MI and 2 had anteroseptal MI. A total 38% i.e. 21 patients had inferior wall MI (IWMI- 42%). Patients with a complicated presentation like malignant arrhythmias and cardiogenic shock had AWMI. Descending order of risk associated with MI in young was alcoholism 40%,Obesity 38%, Metabolic syndrome 38%, HTN 28% DM 26%, IHD 4%, and CKD 4%. (fig 1) Out of 50 patients, most common risk factor is smoking which is 68 %.Females also have risk factors associated with MI.Females have risk in descending order as Obesity and metabolic syndrome followed by HTN, followed by alcoholism then smoking followed by DM. (fig 2)
Table 1: Distribution of cases according to gender
Table 2: Distribution of cases according to age group
Table 3: Distribution of cases according to BMI
Table 4: Distribution of cases according to cardiac Biomarkers
Figure 1 Figure 2 Figure 1: Risk factors in young patients with myocardial infarction; Figure 2: Comparison of Risk factors in young patients with myocardial infarction according to gender
DISCUSSION This was an observational study of clinical profile of 50 patients aged 40 and below admitted with a diagnosis of acute MI. An age cut off of 40 years was selected to define a premature coronary artery disease based on previous epidemiologic studies. The age, gender distribution, the type of clinical presentation, angiographic findings and risk factor distribution were consistent with findings of other related studies. In this study MI in young was found to be more common in males as compared to females. MI in young was distinctly rare in premenopausal women. Also in a study on MI in young, Choudhury L and Marsh 10 have concluded that MI in young is predominantly a disease of men. In our study majority of patients were in the age group of 30 – 40 yrs. In a study done by PA Tambyah et al..11 on premature MI of the 32 patients studied, ages ranged from 32 to 40 yrs. About 25% of acute MI in India occur under the age group of 40 and 50% under the age group of 50. One center reported a 47 fold increase in the incidence of first MI under the age of 40 in the last 20 yrs.12 Majority of patients presented with typical chest pain in this study. In a study done by Lijia Chen et al..13 was concluded that younger patients with coronary artery disease commonly present with an acute coronary syndrome without history of angina. In this study AWMI was most frequent location of MI on ECG. In a study done by PA Tambyah, YT Lim,MH Choo on MI in young AWMI was the most common location of MI . In a study done by P H Stone et al..12 patients with anterior infarction had a substantially worse in- hospital and follow-up clinical course compared with those with inferior infarction, evidenced by a larger infarct size , lower admission left ventricular ejection fraction and higher incidence of heart failure and serious ventricular ectopic activity, in-hospital death and total cumulative cardiac mortality. In this study also AWMI was found in 5 out of 6 patients who had complications like complicated arrhythmias, cardiogenic shock and cardiac arrest. In our study all patients had atherosclerotic changes on CAG, single vessel disease is the most common feature, LAD was most common infarct related artery. In a study done by PA Tmbyah, YT Lim,MH Choo11 on MI in young all patients had evidence of atherosclerotic disease, majority had single vessel disease and LAD was the most common infarct related artery. In another study done by Lijia Chen et al..13, premature coronary artery disease was associated with acute coronary syndromes and complex stenosis morphologic features at angiography. Irregular lesions, filling defects, or both suggesting clot formation or plaque rupture has been recognized by angiography, angioscopy, and autopsy in patients with unstable angina and myocardial infarction. In young MI there is angiographically complex stenosis morphologic features, and less extensive coronary artery disease.14 In this study Smoking, dyslipidemia and metabolic syndrome was the most common risk factor. According to a study done by J Ismail et al.. a majority of young adults with acute MI have at least one identifiable risk factor. The risk factors noted are smoking, diet rich in cholesterol, sedentary lifestyle, diabetes, hypertension, paternal history of cardiovascular disease.2 In this study, prothrombotic states were not a risk factor. Young MI survivors had less severe coronary disease than older patients, which may explain their early favourable outcome. Left ventricular dysfunction would be expected to influence prognosis. It is important not only to diagnose early and treat adequately acute MI in young also it was essential to identify and prevent or treat risk factors at primary and secondary level. Majority of patients in this study were diagnosed with Diabetes, Hypertension. Dyslipidemia after an attack of MI, hence it is important to diagnose and treat these conditions at an early stage before they can lead to such devastating complications. Patients with family history should especially be screened for risk factors. This study also showed metabolic syndrome to be an important risk factor, hence young adults with increased BMI should be screened for other risk factors. There is a need to increase awareness among the young population regarding the entity of MI in young hence stressing on modifying life style in terms of healthy diet, exercise, avoiding smoking and screening for risk factors in those at high risk. This simple measure can make a large difference in preventing the occurrence of MI in young.
CONCLUSION Majority of patients are in 30 – 40 year age group. Majority of young MI patients present with typical chest pain. Anterior wall MI is most frequent location. Single vessel disease was the most common feature. Smoking, dyslipidemia and metabolic syndrome were most common risk factor.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Community Medicine (Print ISSN: 2579-0862) (Online ISSN: 2636-4743) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.