 Home
Home
|
Table of Content - Volume 20 Issue 2 - November 2021
Anterior interrosseous nerve injury in a dumb bell lifter: A case report
P Udhayasingh1*, A Rajakumar2
1Department of PMR, Tirunelveli Medical College, Tirunelveli, Tamil Nadu, INDIA. 2Department of PMR, Madras Medical College, Chennai, Tamil Nadu, INDIA.
Abstract Background: Anterior interrosseous nerve syndrome is a rare compressive neuropathy of upperlimb. AIN is a motor branch of median nerve that innervates pronator quadrates, flexor pollicis longus and radial half of flexor digitorum profundus. The pathophysiology of AIN syndrome could be either a compressive neuropathy or immune mediated neuritis. Management options include non operative conservative management initially; if it is not responsive, surgical management could be tried. Dumbbell lifting usually causes carpal tunnel syndrome. Dumb bell lifting causing Anterior interrosseous nerve syndrome is a interesting presentation The Anterior interrosseous nerve nerve is a major motor branch of median nerve which is important for thumb and hand function. The AIN arises from median nerve, just inferior to elbow and innervates three muscles in the forearm, flexor pollicis lingus (FPL), pronator quadrates(PQ) and radial half of flexor digitorum profundus (FDP). AIN syndrome is a uncommon neuropathy of the upperlimb accounting for only 1% of upper limb nerve injuries3.AIN is a deep seated nerve protected by several structures which makes the AIN lesions rare. These protective structures could be the cause of its compression the Struthers ligament, bicipital aponeurosis, fibrous arches between humeral head and ulnar heads of pronator teres muscles, fibrous arch at the origin of flexor digitorum superficialis, vascular causes such as thrombosis, tumors, hematoma, abscesses, drug injection in to forearm, supra condylar fractures of humerus and proximal third of forearm4.AIN syndrome following lifting is a peculiar and a rare and presented here.
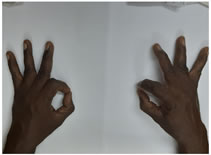
INTRODUCTION A 48 year old diabetic with otherwise no comorbidities presented with complaints of pain in the right thumb associated with weakness of flexion of index finger and thumb for past 3 months. He gives history of dumbbell lifting. He was unable to do OK sign. He was diagnosed to have AIN syndrome and was treated conservatively.
CASE REPORT A 48 year old diabetic male, with no other comorbidities presented to the OPD with complaints of pain in the right thumb associated with weakness of right thumb and index finger for the past three months. He gives history of regularly lifting dumb bell. Physical examination revealed weak flexor digitorum pro fundus of index and middle finger and weak flexor pollicis longus of right hand. He was unable to do OK symbol with thumb and index finger-positive okay sign. Tenderness present 6 cm below the elbow joint. Examination of the peripheral nerve and full musculoskeletal examination including sensation normal. The sensory nerve conduction studies of median nerve shows no abnormalities. Radiographic investigation with Xray of elbow and wrist joints were normal. MRI of forearm revealed hyperintensity signals over FPL and FDP. A diagnosis of Anterior interrosseous nerve syndrome was made and Patient is conservatively managed with rest, analgesia with anti inflammatory agents and physiotherapy for forearm flexor muscle stretching exercises. Patient improved symptomatically by the end of 6 weeks. Figure 1: (Normal left hand) (affected right hand)
DISCUSSION The AIN syndrome is a rare peripheral neuropathy with unclear etiology. It is a rare compressive neuropathy originally described parsonage and Tumor in 19485.The severity and completeness of injury varies substantially, In complete AIN syndrome ,the patient is unable to flex the distal phalanx of thumb and index finger whereas , In incomplete AIN syndrome either the thumb or index finger is affected, due to less axonal damage4.In both cases sensation is not affected. Though AIN syndrome is considered as a compressive neuropathy, there is another theory for its occurrence- an idiopathic immune mediated neuritis6.Ki-tae-na et al. used electrodiagnostic studies and MRI to study the pathophysiology of AIN syndrome and concluded that it could be due to diffuse motor fascicle neuritis of median nerve in the upperlimb7.Clinical presentation includes poorly localized pain in the forearm and cubital fossa with difficulty in bringing the distal phalanx of thumb and index finger together. On doing the pinch test, instead of making okay sign ,the patient will hold the sheet between the index finger and extended thumb. Management of AIN syndrome include is mostly non operative conservative options including a period of rest. Splinting of the elbow in the comfort position of the patient. NSAIDS and physical agent modalities like TENS and NMES can be tried along with stretching exercises of forearm and strengthening exercises of hand and wrist. when the patient not responds to conservative management ,surgical intervention can be tried. Kodama n et al. in their study concluded that when patients show no signs of recovery within 6 months, surgical treatment can be performed within 8 months of symptoms onset. CONCLUSION In our case report, the symptoms and signs of AIN syndrome developed due to muscle hypertrophy or soft tissue changes or stretching of median nerve. Poor diabetic control already weakened the peripheral nerves that got strained by dumb bell lifting. Usually dumb bell lifting causes carpal tunnel syndrome. Dumb bell lifting causing AIN syndrome in a diabetic patient and responding well to conservative management is an interesting presentation.
REFERENCES
Mirko Pham, MD Philipp Bäumer, MD Hans-Michael Meinck, MD Johannes Schiefer, MD
Department of Orthopaedic Surgery, Bahrain Defence Force Hospital-Royal Medical Services, P.O.Box 28743, Riffa, Bahrain
Edie Benedito Caetano a,∗, Luiz Angelo Vieiraa, João José Sabongi Neto b, Maurício Benedito Ferreira Caetano b, Rodrigo Guerra Sabongi c
Lancet. 1948 Jun 26;1(6513):973-8.
Hossein Akhondi; Matthew Varacallo
Narihito Kodama MD, PhD, Kosei Ando MD, PhD, Yoshinori Takemura MD, PhD, and Shinji Imai MD, PhD
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.