 Home
Home
|
Table of Content - Volume 4 Issue 2- November 2016
Study of relationship between DLCO and other spirometric parameters in patients with obstructive and restrictive lung diseases
Luniya A B1, Kapse V R2*, Mhaisekar D G3, Gosavi R A4
1Assistant Professor, Department of Respiratory Medicine, Smt K. N. M. C. and G. H., Narhe, Pune, Maharashtra, INDIA. 2Associate Professor, 3Professor, Department of Respiratory Medicine, Dr S.C.G.M.C. Nanded, Maharashtra, INDIA. 4Assistant Professor, Department of Respiratory Medicine, B. J. M. C. and Sasoon Hospital, Pune, Maharashtra, INDIA. Email: pravin1702@gmail.com
Abstract Background: In diseases such as idiopathic pulmonary fibrosis, the diffusing capacity for carbon monoxide is often decreased out of proportion to the restrictive defect. A DLCO less than 35 to 40 percent predicted for idiopathic pulmonary fibrosis and less than 40 percent for systemic sclerosis has been shown to predict worse outcomes Aims and Objectives: To Study of relationship between DLCO and other Spiro metric parameters. Methodology: The present prospective observational study in patients with obstructive and restrictive lung diseases was approved by the institute ethics committee. Our center has pulmonary unit in a tertiary care government hospital that caters to populations of diverse groups. This is a prospective observational study carried from January 2013 to August 2014. All patients presenting with symptoms of obstructive and restrictive lung diseases lung disease such as breathlessness, cough, chest tightness and wheeze were included. DLCO was done by Jones and Mead technique. Data was entered in the Excel sheets and analyzed. Result: Majority of patients having COPD were in the age group of 45-54 years and 55-64 years, 44.44% and 33.33% respectively. Majority of patients having bronchial asthma were in the age group of 35-44 years 50%. Majority of patients having bronchiectasis were in the age group of 45-64 years 70.00%. Mean age for COPD, Bronchiectasis, Asthma were 55.48yrs, 43.7yrs and 35.72yrs respectively. Amongst ILD patients 17(58.62%) were males and 12(41.38%) were females, male: female ratio in ILD was 1.4:1. Amongst 27 COPD patients 21(77.78%) had decreased DLCO. Amongst 22 Asthma patients 17(77.27%) had increased DLCO. Amongst 10 Bronchictasis patients 8(80%) had decreased DLCO. Amongst 29 ILD patients, 25(86.20%) had decreased DLCO. Amongst 27 COPD patients 21(77.78%) had decreased DLCO. Amongst 22 Asthma patients 17(77.27%) had increased DLCO. Amongst 10 Bronchictasis patients 8(80%). DLCO in patients with COPD decreased progressively with decrease in FEV1 and this graph showing the same. Correlation Coefficient (r=0.94, p<0.001). Conclusion: It can be concluded from our study that Male preponderance is seen in COPD, Asthma, Bronchiectasis and ILD. COPD is common after 35 years of age & as the age increases incidence of COPD increases. Mean age in present study of COPD patients was (55.48yrs). Asthma occurs mostly before 35 years of age. Mean age in present study of Asthma patients was (43.7yrs).DLCO is decreased in the patients with Chronic Obstructive Pulmonary Disease, may be normal or increased in the patients with Asthma and may be normal or decreased in the patients with Bronchiectasis. DLCO is decreased in the patients with ILD FEV1 %predicted correlates positively with DLCO% predicted in patients with COPD. Key Words: COPD, DLCO, ILD, FEV1, Spirometry.
The absorption of oxygen and the elimination of carbon dioxide in the lungs takes place by diffusion and diffusion alone.” August Krogh and his wife, Marie Krogh1: The ability of the respiratory membrane to exchange a gas between the alveoli and the pulmonary blood is expressed in quantitative terms by the respiratory membrane‟s diffusing capacity, which is defined as the volume of a gas that will diffuse through the membrane each minute for a partial pressure difference of 1 mmHg2. Physiologists have devised a variety of methods to study the diffusion of gases across the alveolar-capillary membranes; many of these methods are useful clinically. The advantages of physiologic tests for measuring diffusing capacity are that they permit diagnosis of an impaired surface area for the transfer of gases from the alveoli to the pulmonary capillaries, sometimes even during early stages of disease. Many pulmonary diseases are manifested by a diffusion defect when there is no abnormality apparent in other routine pulmonary function tests3. These diseases include sarcoidosis, asbestosis, scleroderma, lupus erythematosus, emphysema, pulmonary thromboembolism, Pneumocystis jiroveci pneumonia, and rejection of a transplanted lung3. Finally, the tests are relatively simple (as far as the patient is concerned) and easy to repeat, making it practical to study the diffusing capacity frequently and to evaluate the effects of therapy or the natural history of the disease.2 The measurement of pulmonary diffusing capacity requires the use of a gas that is more soluble in blood than in lung tissues. The only gases that have measurable diffusing capacities are those with low solubility in the pulmonary membrane and high capacitance in blood. These gases include oxygen (O2), carbon monoxide (CO), and nitric oxide (NO). Measurement of DL is difficult because, in addition to diffusion, transfer may be limited by other mechanisms, such as ventilation-perfusion mismatching and shunting. The measurement is further complicated by a changing capillary P during capillary transit that cannot be accurately determined4. Carbon monoxide provides an excellent alternative to measuring diffusing capacity because CO normally is present in minimal amounts in blood and binds to hemoglobin in the same manner as . The diffusing capacity measured by carbon monoxide can be converted to that for oxygen by multiplying by 1.23. A low concentration of carbon monoxide is maintained in the air spaces by adding about 0.3% carbon monoxide to inspired air. The mixed venous carbon monoxide concentration is assumed to be zero for all practical purposes (unless the test is repeated frequently over a short time). Molecules of carbon monoxide diffuse across the membrane, dissolve in the plasma, and then combine with hemoglobin. Carbon monoxide has a high affinity for hemoglobin, 210 times that of oxygen; thus, any carbon monoxide in the vicinity of a hemoglobin molecule binds avidly to it and the partial pressure of dissolved carbon monoxide remains very low. Except in a patient with severe anemia, the available binding sites for carbon monoxide are so numerous that3 they cannot possibly be saturated by the number of carbon monoxide molecules that diffuse from the air spaces to the capillary blood at the low concentrations of carbon monoxide used in the test. Therefore, carbon monoxide transfer is not limited by pulmonary blood flow; instead, it is limited primarily by the alveolar-capillary membrane diffusion rate and, to a lesser extent, by the red blood cell membrane diffusion rate and the chemical reaction rate between hemoglobin and carbon monoxide3. In contrast, gases such as Freon, nitrous oxide, and acetylene are equally soluble in lung tissues and blood, because they do not combine chemically with blood components. These gases diffuse across the alveolar-capillary membranes and quickly saturate the plasma; further diffusion is prevented until fresh blood enters the pulmonary capillaries. Thus, these gases can be used to estimate pulmonary capillary blood flow to ventilated lung units. The measurement of DLCO is nearly 100 years old. It was introduced by Marie and August Krogh5 in articles published in 1909 and 1915. Both the single-breath and the steady-state methods have their foundations in these articles. The clinical utility of DLCO did not occur until the infrared carbon monoxide meter was developed in the1940s. This device allowed relatively easy measurement of carbon monoxide, which previously required tedious physical chemistry measurement techniques. Steady state measurements of DLCO have been utilized in some clinical PF laboratories over the years. However, the single-breath method modified by Ogilvie6 has been used for testing in most of the patients.4 The diffusing capacity of the lung for carbon monoxide in a single breath (DLCO), also known as carbon monoxide transference factor (TLCO), is useful in the evaluation of both restrictive and obstructive disease7. The single breath carbon monoxide transfer test is commonly used in differential diagnosis of Chronic Obstructive Pulmonary Disease. A reduction in transfer factor (TLCO) and transfer coefficient (KCO) is the best functional indicator of the presence and severity of pulmonary Emphysema8. The distinction between Asthma and COPD based simply on spirometric parameters is difficult there is a need for more discriminatory test such as lung volumes and DLCO measurements9. DLCO is usually normal or increased in patients with Asthma and decreased in patients of COPD9. A reduced DLCO in the presence of restriction suggests Diffuse Parenchymal Lung Diseases10,11. The diffusing capacity for carbon monoxide (DLCO) may be the first and only abnormality found in the early stages of interstitial lung disease. DLCO can also be used to categorize disease severity12. In diseases such as idiopathic pulmonary fibrosis, the diffusing capacity for carbon monoxide is often decreased out of proportion to the restrictive defect. A DLCO less than 35 to 40 percent predicted for idiopathic pulmonary fibrosis and less than 40 percent for systemic sclerosis has been shown to predict worse outcomes13.
MATERIAL AND METHODS The present prospective observational study was approved by the institute ethics committee. Our center has pulmonary unit in a tertiary care government hospital that caters to populations of diverse groups. This is a prospective observational study carried from January 2013 to August 2014. All patients presenting with symptoms of obstructive and restrictive lung diseases lung disease such as breathlessness, cough, chest tightness and wheeze were included. Also diagnosed cases of Asthma, COPD, Bronchiectasis and ILD were included in this study. Age more than 13 years, Outdoor and indoor patients with obstructive respiratory diseases like COPD, Bronchial Asthma, Bronchiectasis etc. and restrictive respiratory diseases like ILD were included into the study while , Age less than 13 years, Patient unable to perform PFT (due to Neurological, Psychological, and structural disorders), Patients with active pulmonary tuberculosis, Recent myocardial infarction (<1 month) were excluded from the study. Detail clinical examination was done for all the patients. Then all necessary investigations and spirometry were done, in order to confirm the diagnosis of patient. Patients were categorized into Obstructive (Asthma, COPD, Bronchiectasis) and restrictive (ILD) respiratory diseases. Subsequently DLCO in those patients were studied. The investigations like X-ray chest PA view, Sputum for AFB, Complete hemogram including hemoglobin%, complete blood count ECG , HRCT Chest, Spirometry DLCO etc. done. Patients who could hold their breath for 10 sec were posted for DLCO. DLCO was done by Jones and Mead technique. Data was entered in the Excel sheets and analysed.
RESULT Table 1: Age Distribution Of Patients With Obstructive Respiratory Diseases
Majority of patients having COPD were in the age group of 45-54 years and 55-64 years, 44.44% and 33.33% respectively. Majority of patients having bronchial asthma were in the age group of 35-44 years 50%. Majority of patients having bronchiectasis were in the age group of 45-64 years 70.00%. Mean age for COPD, Bronchiectasis, Asthma were 55.48yrs, 43.7yrs and 35.72yrs respectively.
Table 2: Sex Distribution of Patients with Obstructive Respiratory Diseases
Amongst ILD patients 17 (58.62%) were males and 12 (41.38%) were females, male: female ratio in ILD was 1.4:1.
Table 3: DLCO in patients with obstructive airway diseases
Amongst 27 COPD patients 21 (77.78%) had decreased DLCO and 06 (22.22%) had normal DLCO. Amongst 22 Asthma patients 17 (77.27%) had increased DLCO and 05 (22.74%) had normal DLCO. Amongst 10 Bronchictasis patients 8 (80%) had decreased DLCO and 2 (20%) had normal DLCO
Table 4: DLCO in patients with restrictive airway diseases
Amongst 29 ILD patients, 25 (86.20%) had decreased DLCO and 04 (13.80%) had normal DLCO.
Table 5: DLCO in patients with obstructive airway diseases
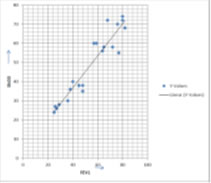
Amongst 27 COPD patients 21 (77.78%) had decreased DLCO and 06 (22.22%) had normal DLCO. Amongst 22 Asthma patients 17 (77.27%) had increased DLCO and 05(22.74%) had normal DLCO. Amongst 10 Bronchictasis patients 8 (80%) had decreased DLCO and 2 (20%) had normal DLCO. Figure 1: DLCO and severity of obstruction in COPD DLCO in patients with COPD decreased progressively with decrease in FEV1 and this graph showing the same. Correlation Coefficient (r=0.94, p<0.001)
Table 6: Over all presentation of dlco in various obstructive and restrictive respiratory diseases
DISCUSSION In present study mean age of the patients for COPD, Bronchiectasis, Asthma and ILD were 55.48yrs, 43.7yrs, 35.72yrs and 61.55yrs respectively. Most patients 26 (96.29%) with COPD were between 35-84 yrs of age and most patients 20 (90.91%) with Asthma were <45 yrs of age. Majority of patients 7(70.00%) having bronchiectasis were in the age group of 45-64 years. Majority of patients, 15 (51.72%), having ILD were in the age group of 45-54 years. Table 7:
In present study amongst COPD patients COPD patients 19 (70.37%) were males and 8 (29.63%) were females, male: female ratio in COPD was 2.4:1. In present study amongst patients with Asthma 13(59.09%) were males and 9 (40.91%) are females, with male to female ratio of 1.4:1. In present study amongst patients with bronchiectasis 6(60%) were males and 4 (40%) were females, with male to female ratio of 1.5. K Jindal Study in COPD15 Male to female ratio of 1.56:1. We found, Amongst 27 COPD patients 21 (77.78%) had decreased DLCO and 06 (22.22%) had normal DLCO. Amongst 22 Asthma patients 17 (77.27%) had increased DLCO and 05 (22.74%) had normal DLCO. Amongst 10 Bronchictasis patients 8(80%) had decreased DLCO and 2 (20%) had normal DLCO. In present study DLCO in patients with COPD decreased progressively with decrease in FEV1 and this the graph showing the same. Correlation Coefficient (r=0.94). This findings correlate with study by Tarek Safwat16, who mentioned that FEV1 %predicted correlates positively with DLCO% predicted in patients with COPD It also coincides with the study by Yaling Zhu17 who stated that Diffusion progressively impaired with severity of COPD. Also B. Brashier, S. Saoji, A. Raghupati, S. Mandrekar18mentions that FVE1 Values correlate positively with DLCO in patients with COPD.
CONCLUSION It can be concluded from our study that Male preponderance is seen in COPD, Asthma, Bronchiectasis and ILD. COPD is common after 35 years of age & as the age increases incidence of COPD increases. Mean age in present study of COPD patients was (55.48yrs). Asthma occurs mostly before 35 years of age. Mean age in present study of Asthma patients was (43.7yrs). DLCO is decreased in the patients with Chronic Obstructive Pulmonary Disease, may be normal or increased in the patients with Asthma and may be normal or decreased in the patients with Bronchiectasis. DLCO is decreased in the patients with ILD FEV1 %predicted correlates positively with DLCO% predicted in patients with COPD.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.