 Home
Home
|
Table of Content - Volume 14 Issue 2 - May 2020
The study on serum lipid profile in children from high risk families
Department of Pediatrics, Indira Child Care, Chennai, Tamil Nadu, INDIA. Email: doctorpriyac@gmail.com
Abstract Background: Atherosclerosis begins in childhood as an accumulation of fatty streaks-lipid-engorged macrophages in the arteries. This commonly causes to increase cholesterol levels which are caused by genetic mutations in lipid and lipoprotein metabolism, acquired conditions. It is noted that interventions to prevent or treat overweight children have had mixed success, with initial positive effects regressing back to and in some cases exceeding baseline. Therefore, it may be better to understand the effect of body mass index on cardiovascular disease risk parameters in school aged children and direct interventions to the most important risk parameters to reduce risk. Materials and Methods: Children of both sexes aged between 9 – 18 yrs are selected, questionnaire, it was analysed in children with no risk factors was selected for the study. Around 2 ml of blood was collected by venepuncture under proper safety conditions after 12 hours of fasting. Lipid profile (Serum Total Cholesterol, Triglycerides, LDL – C, HDL – C and VLDL - C was tested for these children as part of analysis. Results: There is an increase in the moderate risk group children and nearly almost all the children belonging to high risk group elevated lipid fractions. The increasing abnormality of lipid fractions showed good statistical correlation with this method of scoring in which there was a gradual increase in number of risk factors. Statistical significance was seen in respect to total cholesterol (p<0.0018), LDL cholesterol (p<0.043), Triglycerides (p<0.00001), and TC/HDL and LDL/HDL ratios (p<0.00001 and 0.00001) respectively. Conclusion: The study concludes to screen high risk children in a simple manner as possible and assess their total risk and institute cholesterol lowering measures to be taken through the diet pattern strictly and regular exercise must be developed among the children. Key words: Children, cholesterol, high risk
INTRODUCTION Although atherosclerosis manifests clinically in middle and late adulthood, it is well-known that it has a long asymptomatic phase of development, which begins early in life, often during childhood1. In most children, atherosclerotic vascular changes are minor and can be minimized or prevented with a healthy lifestyle. However, in some children the process is accelerated because of risk factors or specific diseases2. Identification of children who are at risk for atherosclerosis may allow early intervention to decrease the atherosclerotic process, preventing or delaying cardiovascular diseases (CVD), such as myocardial infarction, stroke, and peripheral vascular disease 3. Atherosclerosis begins in childhood as an accumulation of fatty streaks-lipid-engorged macrophages (foam cells) and T lymphocytes in the intima of the arteries. Fatty streaks may or may not progress, and may regress4. In some people, lipid accumulation is more pronounced with time, and the accumulated lipid becomes covered by a fibromuscular cap to form what is termed a fibrous plaque. Temporally, between the fatty streak and the fibrous plaque, transitional stages of atherosclerosis exist that are not identifiable by gross examination alone. With time, fibrous plaques enlarge and undergo calcification, hemorrhage, ulceration or rupture, and thrombosis. Thrombotic occlusion precipitates clinical disease such as myocardial infarction, stroke, or gangrene depending on which artery is affected5. Attention was first drawn to the early origin of atherosclerosis by an autopsy study conducted on young soldiers killed in the Korean War. Their average age was 22 years, and over 70% of them had evidence of atherosclerosis in their coronary arteries6. The prevalence of children who are clinical overweight or obsess is increasing rapidly globally. Children and adolescents who are overweight/obese are more likely to be overweight/obese as adults7. In autopsy studies, BMI was positively correlated with more extensive atherosclerotic changes in the aorta and coronary arteries during childhood. Childhood obesity raises the risk of other risk factors that are associated with heart disease in early adulthood, such as high blood pressure or diabetes mellitus8. In one study, children between the ages of 6 and 19 years with metabolic syndrome showed an increased risk of CVD {odds ration: 14.6, 95% confidence interval: 2.8-45.3} at 25 year follow-up compared to the general school population. Generally, overweight children are inactive and may have obstructive sleep apnea, both of which are associated with CVD in adults9. Children and adolescents with hypertension are more likely to have hypertension as adults. In adults, hypertension is a well-established risk factor for CVD that include myocardial infarction and stroke. Although similar direct evidence linking hypertension with CVD is lacking, hypertension has been linked to increased IMT and arterial stiffness, suggestive of accelerated atherosclerosis 10. Dyslipidemia is a disorder of lipoprotein metabolism that results in increased TC, high LDL-C, low HDL-C, and high TG. The National Cholesterol Education Program (NCEP) defines dyslipidemia in children as values that are greater than the 95th percentile and defined cutoff points. Subsequently, the National Health and Nutrition Examination Surveys (NHANES) presented age- and gender-specific lipoprotein threshold concentrations for adolescents. The predictive capacity of both NCEP and NHANES cut points were similar predicting high common carotid artery IMT in adulthood11. Adolescent lipid levels were more strongly associated with high IMT in adulthood than change in lipid levels. Overweight or obese adolescents with dyslipidemia had increased cIMT in adulthood compared with those who did not have both risk factors, leading the authors to suggest that dyslipidemia screening could be limited to overweight or obese adolescents12. Although dyslipidemia is an established risk factor for CVD in adults, no long-term studies directly link dyslipidemia in childhood with subsequent CVD, with the possible exception of children with monogenetic causes of dyslipidemia such as familial hypercholesterolemia. Autopsy studies demonstrated an increase atherosclerotic lesions in the coronary artery and aorta with increasing serum LDL-C and decreasing HDL-C. Individuals who displayed elevations in non-HDL-C, LDLC, and TC: HDL-C in children are more likely to have increased IMT in adulthood13. Abnormal cholesterol levels are commonly caused by genetic mutations in lipid and lipoprotein metabolism, acquired conditions (e.g., high fat, high carbohydrate diet, lack of exercise, obesity, and a variety of medications), or both14. Although lifestyle related dyslipidemias are common, genetic mutations that alter regulatory mechanisms of lipid and lipoprotein metabolism, such as FH, pose a unique concern. Because elevated cholesterol is present from birth, FH results in lifelong elevation of LDL-C, significantly increasing the risk of premature cardiovascular disease in childhood. Universal screening of all children starting at age 9–11 is currently recommended all over world, the literature suggests that high levels of LDL-C can be accurately detected in much younger children.15 Diagnostic thresholds of LDL-C likely vary by age. Levels of both total and LDL-C show considerable overlap between adults with and without FH, making detection through screening more effective in children. Detection at a young age offers opportunity for early intervention of the child and affected relatives through RCS. Several screening strategies have been proposed to identify individuals with elevated LDL-C who are at high risk for premature CVD (16). These include targeted screening of individuals based upon family history and/or known CVD risk factors, universal screening, cascade and reverse cascade screening of relatives of individuals found with either early CVD or LDL-C consistent with FH, and big data approaches to identify persons with high cholesterol and risk of premature CVD. Because affected children are asymptomatic, often of normal weight, and the family history is either unavailable, incomplete, or unreliable, systematic universal screening is recommended to facilitate early identification of children and adolescents with hypercholesterolemia 17. Childhood obesity has been linked to a 12 fold increase in fasting insulin concentration in obese children aged five to 17 years. In addition, amounts of triglycerides, total cholesterol, low density lipoprotein cholesterol (LDL cholesterol), and high density lipoprotein-cholesterol (HDL cholesterol) are all more likely to be abnormal in overweight children than in normal weight children. Risk parameters for cardiovascular disease in childhood such as body mass index, cholesterol, blood pressure, and triglyceride concentrations have shown to be significantly correlated with adult levels over long term follow-up. Furthermore, raised risk of cardiovascular disease has been found as well as increased coronary heart disease events over a five million person year follow-up. Therefore, childhood health could greatly affect the risk of cardiovascular disease in adulthood18. Studies that have focused on interventions to prevent or treat overweight children have had mixed success, with initial positive effects regressing back to and in some cases exceeding baseline. Therefore, it may be better to understand the effect of body mass index on cardiovascular disease risk parameters in school aged children and direct interventions to the most important risk parameters to reduce risk19. However, to our knowledge, there has been no study on studying the risk factor of early development of arteriosclerosis in high risk families with coronary artery disease, incidence of hyperlipidemia, systematic examination of the magnitude of the relationship between body mass index categories and sex on risk parameters for cardiovascular disease in school aged children20. It is proposed to study by screening the lipid profile in children of high risk families as risk factor for the early development of atherosclerosis and coronary artery disease. The incidence of hyperlipidaemia in children of high risk group will be evaluated. The relationship of body mass index to hyperlipidemia is also studied in this study. Thus an attempt is made to study the above in detail in school children which can benefit their future. Subject selection Children of both sexes aged between 9 – 18 yrs are selected for the study. The questionnaire used in this study is developed by the author and validated. This is used to identify the high risk families. High risk is defined as family history of hypertensions, premature coronary artery disease, hypercholesterolemia, strokes and diabetes. All the questionnaires analysed 100 children were shortlisted with no risk factors was selected for the study and 100 children were identified for control. Around 2 ml of blood was collected by venepuncture under proper safety conditions after 12 hours of fasting. Lipid profile (Serum Total Cholesterol, Triglycerides, LDL – C, HDL – C and VLDL - C was tested for these children as part of analysis.RESULTS Figure 1 Figure 2 Figure 3 Figure 1: The age distribution (9 -12 yrs, 13 – 15 yrs and 16 – 18 yrs) in years, this study Age Distribution – Sex wise; Figure 2: The age distribution (9 -12 yrs, 13 – 15 yrs and 16 – 18 yrs) sex wise, this study; Figure 3: The prevalence of risk factors this study
Table 1: The different risk groups in this study with abnormal lipid fraction
Table 2: The Abnormal Lipid Fractions – Distribution
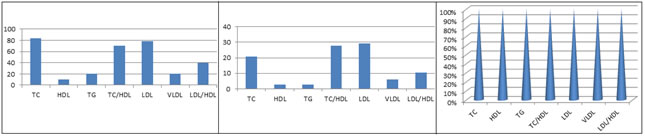
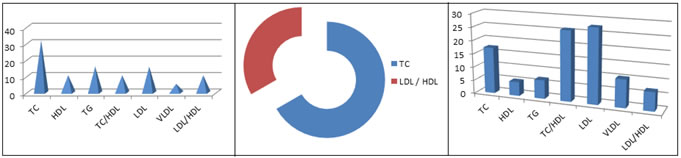
Abnormal lipid profile distribution Figure 4 Figure 5 Figure 6 Figure 7 Figure 8 Figure 9 Figure 4: The Abnormal Lipid Fractions – Distribution; Figure 5: Relationship of Abnormal Lipid Fractions to Hypertension; Figure 6: Relationship of Abnormal Lipid Fractions to Cardiac Disease; Figure 7: Relationship of Abnormal Lipid Fractions to Stroke; Figure 8: Relationship of Abnormal Lipid Fractions to Hyper cholesterolemia; Figure 9: Relationship of Abnormal Lipid Fractions to Hypertension and Cardiac Disease. Table: 3 - Association of Lipid Profile with scored risk factors
DISCUSSION The risk of coronary artery disease is on the increase in developing countries and Indians as a race seem to be genetically prone for the same. It has been well established that persistence of elevated levels of total cholesterol from childhood to adolescence together with identifiable factors like lifestyle, personal habits at risk and a positive high risk family history can together be sensitive pointers for the early detection of cardiovascular risk of coronary artery disease21 Western literature seems to be abounding in many perceptive and retrospective studies to find out the correlation between these factors and CAD, but Indian studies are very sparse and seem to concentrate on a single factor like obesity or smoking or hypertension in relation in CAD, hence the need for this study which taken into account a conglomeration of risk factors22. This study screened children at high risk and conclusively showed that the total serum cholesterol and LDL – cholesterol were both positively influenced by various adverse risk factors like obesity, lack of exercise, family history of hypertension, CAD strokes23. Over the decades, epidemiologic, metabolic ward, animal experimental, clinical trial, anthropologic, and other research modalities have produced extensive concordant knowledge on the disturbances of human culture, first and foremost dietary—that caused epidemic CHD. The crucial scientific findings to end the CHD epidemic are now available. The challenge and task is to apply them in all appropriate patient contacts and across all population strata to extend the progress to date24. One key for achieving this is priority emphasis on primordial prevention, ie, family dedication to favourable lifestyles (nutrition, exercise, nonsmoking) as norms of human behavior. This especially applies to the future mother so that when she conceives and throughout pregnancy, her exposures and those of her fetus are optimal and become primary and lifelong habits for the newborn infant and preschool child. Healthy eating patterns such as the DASH (Dietary Approaches to Stop Hypertension) diet are available as models for this crucial aspect of disease25. The genetic factor is supposed to be the leading factor when CAD presents early in life. Several studies have documented the association between cholesterol levels and prevalence of CAD. The association between CAD and levels of cholesterol is complex to estimate in children because clinically significant CAD does not happen 26, 27. In the current study, the children of parents with CAD have a significant occurrence of hyperlipidemia and there is an association between lipid profile levels of children. It was reported that 72 children whose ancestors had myocardial infarction had increased levels of cholesterol; however, there was no significant difference in levels of triglyceride. It was reported that there was an association among lipid profile levels of parents and their children with total cholesterol levels. This study is similar to other studies. Increased levels of serum cholesterol, triglycerides and LDL are several of the significant factors in these patients. It was reported that hypercholesterolemia is common in children of parents with recognized hypercholesterolemia and symptomatic coronary artery disease 28. An increased total cholesterol along with HDL ratio influences primary coronary artery disease. This ratio in the current study of high risk children was significantly more increased than the ratio given by earlier workers. It has been revealed that the entire risk factor separately enhances the risk of coronary artery disease by 5 to 10 times compared with having no risk factors 29. The present study observed the lipid profile in children with CAD compared to the control group. High levels of cholesterol and triglyceride and low levels of HDL and LDL in children with CAD were found. Our results conclude that it is useful to monitor the lipid profile of children of parents with coronary artery disease. Children of parents with CAD and hyperlipidemia are at high risk of progression to premature atherosclerosis and need lipid profile assessment monitoring. The lipid profile of children diagnosed with intermittent major risks can be taken to reduce these risks. Further studies with greater sample numbers are necessary to confirm these findings 30. There are more than 40% of high risk families were identified and 35% of children studied had abnormal lipid fractions. The family risk factor is due to abnormal lipid profile, TC and LDL – Cholesterol. These are good indicators which can identify children at risk for early coronary artery disease. Blood Cholesterol Levels in Children and Adolescents specify positive family history in biological parents and grandparents for CVD as myocardial infarction, angina pectoris, peripheral or cerebral vascular disease, sudden death, coronary artery bypass-surgery or balloon angioplasty before age 55 (31). It should be noted that in children CVD risk we evaluate medical history of first and second-degree relatives. The most remarkable result of our study is significant increase of TG and VLDL serum concentration in children aged 1.5-2.5 years with a family history of premature CAD compared to controls. However we did not find any differences in lipid profile in newborns with a positive family history of premature CAD and controls. Kelishadi et al. reported a significantly higher levels of TG, TC and LDL, and lower levels of HDL in children of parents with premature CAD. Romaldini et al. showed hypercholesterolemia in 27.5% and hypertriglyceridemia in 12.8% of children of high-risk families. In young adults aged 19 -30 years with parental premature CAD only TC concentration was significantly higher than in controls. Marcovecchio et al. reported significant differences regarding TG and HDL between adolescents with a history of parental dyslipidemia and non-risk controls32. Mendes et al. revealed higher values of TC and lower of HDL in offspring of young adults with CAD than in controls. It should be noted that our study was conducted only in children aged 1.5-2.5 years and most of mentioned studies were performed among older children and adolescents. Lipids and lipoproteins concentrations are the lowest during intrauterine life and at birth, and then increase until 2 years of age. Human lipid levels became quite constant up to adolescence. Moreover, to understand some of these differences the ethnic and racial disparities should be also taken into consideration 33. Elevated Lp(a) levels have been identified as independent risk factor for CAD that promotes atherogenesis and thrombogenesis. Several studies in children have found a positive association between Lp(a) level and positive family history of CVD. This concept has been challenged by Tonstad et al. demonstrating that Lp(a) was marginally lower in the children with a history of premature cardiovascular death in relatives 34. Thus screening of high risk children is very important in this current scenario. They should be properly followed up with the regular diet pattern. It was noted that all the lipid values were significantly higher in children of parents having CAD compared to control in the study done by S K Chugh 37. In the present study it was noted that the total cholesterol and LDL cholesterol were significantly elevated and showed good statistical correlation in the presence of parental risk factors. It was also noted that HDL – C was found to be less significant and only 7% of children showed no significance. There was no correlation between hypercholesterolemic children and passive smoking. The outcome of the correlation showed that only few children had family of smoking history. The children in the study followed a vegetarian diet. There was lack of exercise in most of these children thus contributing obesity in a significant proportion. Another important finding in this study is hypercholesterolemia increased in direct proportion to the number of risk factors present. In the presence of a single risk factor it was noted that abnormal lipid profile was seen is 33%. When two risk factors were identified, hyperlipidemia rose to 48%; 59% of children who had family history of hypercholesterolemia in association with other risk factors had elevated lipid fractions indicating that presence of hypercholesterolemia in the family. Analysing the various lipid fractions in relation to the scoring pattern devised, it was noted that 17% of the children who belonged to the low risk group had abnormal lipid fractions 35. The abnormality increased to 76% in the moderate risk group children and nearly almost all the children belonging to high risk group elevated lipid fractions. The increasing abnormality of lipid fractions showed good statistical correlation with this method of scoring in which there was a gradual increase in number of risk factors. Statistical significance was seen in respect to total cholesterol (p<0.0018), LDL cholesterol (p<0.043), Triglycerides (p<0.00001), and TC/HDL and LDL/HDL ratios (p<0.00001 and 0.00001) respectively.
CONCLUSION Furthermore this study shows that the need of the hour is to screen for these high risk children in a simple manner as possible and assess their total risk and institute cholesterol lowering measures to be taken through the diet pattern strictly and regular exercise must be developed among the children. The avoidance of smoking with the parents needs to be emphasized. These children should be followed up at yearly intervals and interventions should be modified accordingly.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.