 Home
Home
|
Table of Content - Volume 15 Issue 1 - July 2020
Clinical profile of Rickettsial fever in children in a government tertiary care institute in north Karnataka
Vishwanath Pattar1, Venkatesh G2*, Shantharaja G C3, Srinivasa Arer4, Jayaraj Pati5, Shivanagouda J6
1,3DCH(CPS Mumbai)Post Graduate, 2Assistant Professor, 4Professor & HOD, 5,6Associate Professor, Department of Paediatrics, Gadag Institute Medical Sciences Gadag, INDIA.
Abstract Background: Rickettsial diseases are a group of Febrile illnesses caused by obligate intracellular gram negative coccobacilli and transmitted to man by arthropod vectors., often under diagnosed due to poor awareness. Rickettsial Diseases are dangerous among children, due to atypical presentations and complications, as increasing trends in India since last many years. Objective: To assess the clinical Profile of Rickettsial fever among Children. Methodology: A prospective Cohort study was conducted in the Dept of Pediatrics, Gadag Institute of Medical Sciences Gadag Karnataka State, among the Children Attended OPD and Admitted in our Hospital, from the month of September 2019 to February 2020, a total of 131 cases reported during the study period have been included. Results: All cases Having H/O High grade Fever and Weil Felix anti body test, positive [131- 100%] have been included. Among them 49 {39%} are positive for Spotted fever(OX-2) [ caused by Rickettsia ricketsii, conori], 22{17%} for Scrub typhus(OX-K) [ caused by Orienta Tsutsugamushi], 22 {17%} for Endemic Typhus/Epidemic typhus (OX-19) [caused by Rickettsia Typhi, prowazeki], 27 { 21%} for both scrub Typhus and Endemic Typhus, 7(5%) for both Scrub typhus and spotted fever, 1(0.78%) for both Endemic typhus and Spotted fever, 3(2.2%) for all 3 antigens. All the cases have been treated with Doxycycline 2.8-3mg/kg/day BID doses for 7 to 10 days. Among them about, 33% patients responded within 48 hours of treatment, 57% within 72hours 10-12% , recovered well within 5-6days of the treatment. Conclusion: Rickettsial fever does exist in our area and incidence is rising after the ending of rainy season peak during the month of September to January. Rickettsial fever should be kept in mind for workup of exanthematous fever. Keywords: Rickettsial fever, Exanthematous fever, Weil Felix anti body test, Febrile illnesses.
INTRODUCTION Rickettsial diseases are a group of Febrile illnesses caused by obligate intracellular gram-negative coccobacilli and transmitted to man by arthropod vectors., often under diagnosed due to poor awareness.1,2,3 In recent years outbreaks have been reported in the sub Himalayan Belts, Maharashtra, Rajasthan, Punjab, Tamil Nadu, Kerala, Karnataka4,5,6,7,8,9 and Rickettsial diseases are important and often under recognized cause of febrile illnesses in children with wide variety of atypical multisystem clinical manifestations.10,11 The family of Rickettsia is named after HOWARD TAYLOR Ricketts who discovered Spotted fever and died during his studies in 1909.12,13 Rickettsial are group of motile, gram negative, non-spore forming, highly pleomorphic bacteria present as coccobacilli, or thread like intracellular obligate parasites., divided epidemiologically into 4 groups.1,2
Spread by Arthropod vectors, lice, fleas, ticks, mites are the most frequent presenting symptoms include, high grade fever, headache, rashes, myalgia, anorexia, nausea, vomiting, diarrhea, abdominal pain., and complicated cases may have multi organ involvement -encephalopathy, pulmonary edema, acute renal failure, vascular collapse, myocarditis, hepatic failure.1,2,13,14 Rickettsial Diseases are dangerous among children, due to atypical presentations and complications, as increasing trends in India since last many years.2,13,14 We in the north Karnataka zone met across with more endemic cases of Rickettsial diseases, coming from rural and urban areas of Gadag district, in the month of September and October, as we don’t have much study data on Rickettsial fever in our District area, thus we conducted a study to evaluate the disease presentation, profile and prevalence of organism causing disease, among children attended OPD and admitted in our hospital. This study aims clinical suspicion, awareness about transmission, and laboratory evaluation, treatment and
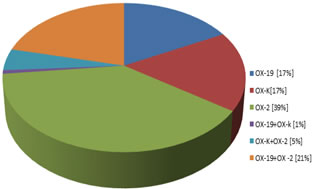
METHEDOLOGY A prospective Cohort study was conducted in the Dept of Pediatrics, Gadag Institute of Medical Sciences Gadag Karnataka State, among the Children Attended OPD and Admitted in our Hospital, from the month of September 2019 to February 2020, a total of 131 cases reported during the study period have been included. Base line Data of age, sex, local residing area, exposure to animals , Socio economic status, date of admission, days onset of first symptom fever/ rash , distribution of rash, associated other systemic co morbidities, were recorded, and done CBC of all patients, weil Felix test to identify the type of species, Procedure of weil Felix test The Weil-Felix test is based on the detection of antibodies to various cross-reacting Proteus antigens with Rickettsia (Proteus vulgaris OX2 with spotted fever Rickettsiae, P. vulgaris OX19 with typhus group Rickettsiae and Proteus mirabilis OXK with O.Tsutsugamushi). The Weil-Felix test was performed on all the serum samples collected at the time of presentation at the hospital (acute sample)13 Done by Slide test method using with PROGEN- Proteus antigen suspensions for weil Felix test. [Manufactured by TULIP DIAGNOSTICS (P) LTD, Verna Goa.] packed with 3 separate containers of 5ml of Reagents of OX-K [scrub typhus], OK-19 [epidemic typhus] and OX-2 [scrub typhus]. A clean white background reaction circle glass slide is taken, place one drop of Positive control, physiological saline, and patient serum to be tested in each circle of the slide, then put 1 drop of appropriate PROGEN antigen to each circle, mix with separate mixture sticks wait for 1 minute, and see the level of agglutinins in serum circle, positive agglutinins indicates presence of Rickettsial antibodies in the patient serum, Agglutination titer of 1:80 or more was considered significant for Rickettsial infection. And also we done LFT, RFT, Serum electrolytes, peripheral smears, dengue card test, for necessary patients, and treated with Doxycycline 2.5-3 mg/kg BD doses for 7-10 days. INCLUSION CRITERIA Clinically suspected cases with h/o fever, macula popular, Erythematous rash, in children with age group of 6months to 18years with Positive weil Felix test for - OX-19, OX-2, and OX- EXCLUSION CRITERIA Fever and Rashes with Dengue Positive, Leptospirosis, Brucella infections Statistical Analysis: Data was entered in Microsoft Excel and analyzed using SPSS version 24.0th. Mean and Standard deviation were calculated for quantitative variables, and proportion calculated for categorical variables. Ethical committee approval taken from Institution.RESULTS In our study duration of 6 months, from Sep2019 to Feb 2020, included 131 [51 OPD (38.9%) + 80 IPD (61.01%) Cases] children of age group 6 months to 18 years, in which 71 are Male (54.19%) 60 are Female (45.81%). Highest Burden of the disease occurred during Sep and Oct months [71 cases 54.19%] soon after rainy season, among them 48 Cases [36.9%] have h/o animal contact [Dog, goat, cow, Buffalo, and insect bites; Rat flea], 12cases [9.1%] have h/o Lice infestation. All cases Having H/O High grade Fever and Weil Felix anti body test, positive [131- 100%] have been included. Among them 49 {39%} are positive for Spotted fever(OX-2) [ caused by Rickettsia ricketsii, conori], 22 {17%} for Scrub typhus(OX-K) [ caused by OrientaTsutsugamushi], 22 {17%} for Endemic Typhus/Epidemic typhus (OX-19) [ caused by Rickettsia Typhi, prowazeki], 27 { 21%} for both scrub Typhus and Endemic Typhus, 7 (5%) for both Scrub typhus and spotted fever, 1(0.78%) for both Endemic typhus and Spotted fever, 3(2.2%) for all 3 antigens. 84 cases [64.1%] have Purpuric Rashes, Hepatomegaly 23 [17.5%], GI Upset 78 [59.5%], Seizures and Encephalopathy 5 [3.8%], Malaise, Body ache 42 [32%], Cough and Pneumonia 46 [35%] are present. Distribution of Prevalence of Type of Rickettsial species is shown in the Pie Chart below. Figure 1: Weil felix test interpretation
The following Table no 1 shows multi systemic clinical manifestations of the reported cases and Table no 2 shows Laboratory investigations. Table no 3 other lab investigations
Table 1: Major Presenting symptoms
Table 2: Lab investigations
Table 3: Other Lab investigations
DISCUSSION Rickettsial Diseases are one of the important cause for Febrile illnesses in children with wide variety of clinical manifestations, often under diagnosed due to poor awareness. In our study we have shown the disease profile and prevalence of type of Rickettsial species [strain] in our area. In our study age group ranged from 6months to 18 years, with mean age of 7.5 year, with no statistically significant sex difference. Which is similar to Kalal B S14, 6months to 12 years taken mean age 7.4 years and Sunil S. Vaidya13, <18 years with mean age 7years. All the patients presented with fever[100%], Maculopapular purpuric rashes seen in 64%, which is 82% in Sunil S Vaidya13, 36% in Kalal B S14, GI symptoms, 59.5%, which is 25% in Sunil S Vaidya13, 44% in Kalal B S14, Hepatomegaly 17.5%, which is 65% in Sunil S Vaidya 13, 71% in Kalal B S14, CNS symptoms 3.8%,,which is 34% in Sunil S Vaidya13, 15% in Kalal B S14, Resp symptoms 35%,,which is 5% in Sunil S Vaidya13, Headache/malaise 32%, which is 10% in Sunil S Vaidya.13 In our Study found, Leukocytosis 36.6%, which is 66% in Sunil S Vaidya13, Thrombocytopenia 20%, which is 56% in Sunil S Vaidya.13 In our Study according to Weil felix test among {39%} are positive for Spotted fever[ caused by Rickettsia ricketsii, conori], is prevalent in our area, 22 {17%} for Scrub typhus [ caused by Orienta Tsutsugamushi], {17%} for Endemic Typhus/Epidemic typhus [caused by Rickettsia Typhi, prowazeki], 27{21%} for both scrub Typhus and Endemic Typhus, whereas Tick born spotted is or epidemic typhus is prevalent in in Sunil S Vaidya13, and Scrub typhus 85.5%, 37.1% Spotted fever in in Kalal B S14, Scrub typhus 80% in Thomos R, et al.15 As the weil felix test may give false positive cross reaction with proteus species, leptospira, Borelia infections, a definitive test like ELISA or PCR should be done to confirm the specific Rickettsial strains. In some study centers used Chloramphenicol or Doxycycline for treatment; we used only Doxycycline and are responded well in all the cases.
CONCLUSION Rickettsial fever does exist in our area and incidence is rising after the ending of rainy season peak during the month of September to January. Rickettsial fever should be kept in mind for workup of exanthematous fever. Early diagnosis and treatment with Doxycycline can reduce the hospital stay and cost. Use of Empherical treatment may be considered to reduce the morbidity and mortality observed with the disease. Limitation of the study As the Weil Felix test not Diagnostic standard, it should be interpreted in good clinical context, still easily available to all and remain good screening test. Investigation like PCR should done to detect and Strengthen the diagnosis of Rickettsial organism.
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.