 Home
Home
|
Table of Content - Volume 16 Issue 1 - October2020
Askin’s tumour- A rare case presentation
Kakulavaram Animisha1*, Mrunalini Kulkarni2
1Intern, 2Associate professor, Department of Pediatrics, Bharati Vidyapeeth (deemed to be university), Sangli, Maharashtra, INDIA Email: animisha.kvr@gmail.com
Abstract Askin’s tumor is form of primitive neuroectodermal tumor developing from the soft tissues of the chest wall1. Here, we present a case of Askin’s tumour in a 5-year-old male child who had presented with swelling and pain over left anterior chest wall. Small biopsy of the mass was done which confirmed the diagnosis. Key Word: PNET. Askin’s tumor.
INTRODUCTION Askin's tumor is a peripheral primitive neuroectodermal tumor within the thoracopulmonary region, which primarily occurs in children and young adults. It is a highly misdiagnosed and rare disease with a lack of clinical and pathological morphology in nature, which is easily confused with other small round-cell tumors2.
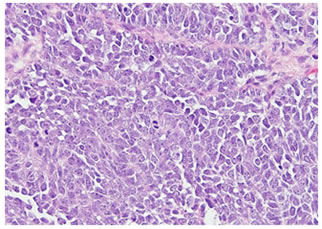
CASE PRESENTATION A 5 year old male child presented with swelling over left anterior chest wall in the 4th ICS and fever since 15 days. Swelling was associated with pain and was gradually increasing in size. He had no history of cough, breathlessness, hemoptysis, trauma. On examination, the patient was afebrile with pulse rate of 96/min, RR of 42/min and BP of 100/66 mmHg. Mild pallor was present and SpO2 was 97% at 3 litres of O2. Grade I clubbing was present. On Local examination, a tender hard mass of size 4x4 cm was palpable superolateral to left breast. On Auscultation, Breath sounds were reduced in left infraclavicular and mammary area. Bronchial breath sounds were heard in left mammary area. Lab investigations included CBC which revealed Hb- 11.1, WBC- 11300, Platelets- 4,67,000, ESR-40 (raised). LFT, RFT and Electrolytes were normal. LDH- 639 (raised). Chest X-ray revealed mass in between left 4th and 5th ICS with pleural effusion and lung collapse. Diagnostic pleural tapping was done which revealed hemorrhagic fluid. CT chest with contrast revealed left pleural effusion with left lung collapse. Mass lesion of size 5cm was noted in pleural space extending to extra-thoracic muscle plane. Small biopsy- of mass of left chest revealed malignant small round cell tumor suggestive of Askin’s tumor (PNET). The patient was referred to higher centre for further management. Figure 1: Histology Slide- Askin’s tumor showing small round cells
DISCUSSION Peripheral primitive neuroectodermal tumor (PNET) is a type of soft tissue sarcoma, described as arising intracranially2. PNETs arise from the primitive nerve cells of the nervous system, but they can also occur outside the central nervous system (peripheral PNETs) in the chest wall, pelvis, extremities and so on3. PNETs of the chest wall were originally reported by Askin et al in 1979, since then, a PNET that occurs within the thoracopulmonary region is named as Askin's tumor. It has been reported to primarily occur in children and young adults2. It is a subset of Ewing sarcoma which arises from the chest wall. Histologically, it is distinguished by typical small round blue cells of monomorphous appearance. It is more frequent in males than infemales (1.5:1)5. This disease primarily occurs in the soft tissue of the chest wall, rib periosteum, chest and lung2. Askin’s tumor usually presents with common respiratory symptoms. It may include symptoms like cough, chest pain, fever and breathlessness5. The commonest radiographic manifestation is a chest wall soft-tissue density mass, sometimes associated with rib erosion and/or pleural effusion4. Treatment of Askin's tumor consists of radical surgery, neo-adjuvant or adjuvant chemotherapy and radiotherapy. The best prognosis can be provided by surgical treatment with wide resection. As local recurrences after resection and metastases are frequently seen in Askin tumor, it has a poor prognosis and a short survival6.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.