 Home
Home
|
Table of Content - Volume 16 Issue 2 - November 2020
Evaluation of febrile seizures in iron deficiency anaemia among children in western Rajasthan
Nimish Khatri1*, Madan Gopal Choudhary2, Shaina Raheja3
{1,2Assistant Professor, Department of Paediatrics} {3Medical Officer, Department of Pathology} S. P. Medical College, Bikaner -334003, Rajasthan, INDIA. Email: khatrininmish@gmail.com
Abstract Background: Febrile seizures are the commonest cause of seizures in children. In developing countries malnutrition and anaemia are commonly associated comorbidity. Interrelation of febrile seizures and iron deficiency anaemia is evaluated. Method: This case control study evaluated 300 children aged 6 to 60 months and these were divided in two groups. Each group included 150 children. One group had febrile seizures and another group was febrile but without seizures (control). Both groups were compared. Results: The mean value of Hb (gm/dl) in febrile seizure group was 9.02 (SD±1.50) and in control group it was 10.57 (SD±1.40), t test value was 6.50 p<0.01. Mean value of Hematocrit (Hct %) in febrile seizure group was 29.3(SD±4.02) and in control was 32.2 (SD±3.60) t=6.42 p<0.01. RDW (fl) mean value in febrile seizure group was 44.4 (SD±2.60) and in control group was 42.1 (SD±3.14), t=6.91 p<0.01. MCV (fl) mean value of febrile seizure group was 69.5 (SD±5.90) and in control was 74.3 (SD±6.90) t=6.36 p<0.01. MCH (pg) mean value of febrile seizure group was 22.3 (SD±3.20) and in control group was 24.1 (SD±3.05) t=4.98 p<0.01. Mean MCHC (gm/dl) value of febrile seizure group was 30.2 (SD±2.12) and in control was 31.4 (SD±1.30) t test – 5.91 p<0.01. The serum ferritin (ng/ml) mean value in febrile seizure group was 40.8 (SD±19.2) and in control group was 65.9 (SD±25.4) t = 9.6 and p<0.01. Conclusion: This study highlights the relation of Iron deficiency anaemia in febrile seizure. Haemoglobin carries Iron to every part of body including brain hence its deficiency will have reactive phenomenon like febrile seizure because of impairedneuro transmitters. Keywords: Febrile seizures, Iron deficiency anaemia, Haemoglobin, Serum Ferritin, Chemi Luminescence Immune Assay.
INTRODUCTION Febrile seizure (FS) is the most common convulsive disorder in children amounting to 2-5% of children aged between 6 to 60 months1.Although FS is mostly benign but rarely leads to brain damage. It may cause emotional, physical and mental changes in children which are stressful, worrisome for parents and affects their quality of life2,3. Majority of the studies have reported that Iron Deficiency Anaemia (IDA) has significant role in FS. Iron deficiency anaemia is more common in children under 2-3 years of age and FS are also common in the same age group. Due to presence of Iron in haemoglobin it plays a crucial role in the transport of oxygen to different tissues of the body such as brain4.Iron deficiency (ID) reduces the metabolism of some neurotransmitters such as monoamine and aldehyde oxidase5. The studies carried out in different regions have given different results about relation of iron deficiency anaemia with FS. Some studies have reported the higher incidence of FS in IDA and on the contrary some authors have mentioned that risk of FS in IDA children is less and ID can be a protective mechanism against convulsions by increasing the seizure threshold and thus iron supplements should be given with caution to the children6. Some studies say that ID has no role in FS7,8. Considering above conflicting reports the present study was conducted in our region to compare the role of IDA in the FS to those in febrile patients without seizures.
MATERIAL AND METHODS Three hundred patients aged between 6 months to 60 months admitted at paediatric ward of S. P. Medical College and associated group of hospitals, Bikaner, Rajasthan were studied. Inclusive Criteria: Paediatric patients having simple febrile convulsion and patients presenting with short duration of fever (<4 days) but without seizures were selected for study. Exclusion Criteria: Children with complex febrile seizures, children with family historyofepilepsy, mental retardation and severe malnutrition were excluded from the study. Methods: This case control study evaluated 300 children aged 6 to 60 months and these were divided in two groups. Each group included 150 children. One group had febrile seizures and another same age group were febrile but without seizures (control). Both groups were compared. Each patient was evaluated for Hb, HCT, MCV, MCH, MCHC, RDW, PS (peripheral smear) examination. Serum ferritin level was estimated in both the groups. Red Blood Cell (RBC) indices were estimated using an automated haematology analyzer (Sysmex kx-21) and serum ferritin estimation done using chemi luminescence immune assay (Advia centaur-Fully Automated). Febrile seizures(9) were diagnosed as per ILAE classification and diagnosis of IDA was done as per guidelines by WHO 10. The duration of study was two years(January 2018 to January 2020). Statistical analysis: Fever with seizure group and fever without seizure (control) group reports were compared by SPSS software using Z test.
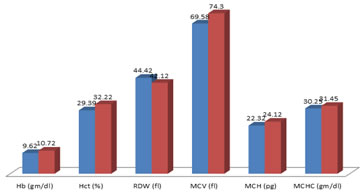
OBSERVATION AND RESULTS Table-1and Graph-1 shows comparison of haematological profile in simple FS and control group. In FS group mean Hb (gm/dl) value was 9.62 (SD±1.50) and in control group was 10.72 (SD±1.40) t test value was 6.50, (p<0.01). Mean Hct(%) value of FS group was 29.39 (SD±4.02) and in control group was 32.22 (SD±3.60) t test value was 6.42,(p<0.01). Mean RDW(fl) value in FS group 44.42 (SD±2.60) andin control group 42.12 (SD±3.14) t test value was 6.91, (p<0.01). Mean MCV (fl) value in FS group was 69.58 (SD±5.90) andin control group was 74.30 (SD±6.90) t test value was 6.36, (p<0.01). Mean MCH(pg) value in FS group was 22.32 (SD±3.20) and in control it was 24.12 (SD±3.05) t test value was 4.98 , (p<0.01). Mean MCHC (gm/dl) value in FS group was 30.25 (SD±2.12) and in control group was 31.45 (SD±1.30) t test value was 5.91, (p<0.01). Table-2and Graph-2shows comparison of serum ferritin (ng/ml) in both groups, mean value in FS group was 40.8 (SD±19.2) and in control group it was 65.92 (SD±9.6) t test value was 9.6, (p<0.01).
DISCUSSION In the present study the mean Hb (gm/dl) value in febrile seizure group was 9.62 (SD±1.50)and in control group was 10.57 (SD±1.40) t test value was 6.50 and p value was highly significant (p<0.01). Mean HCT(%) value in febrile seizure group was 29.3 (SD±4.02) and in control group it was 32.2( SD±3.6) t test was 6.42 p<0.01. Mean RDW (fl) value in febrile seizure group 44.4 (SD±2.60) and in control group it was 42.1 (SD±3.14), t test was 6.91 p<0.01. Mean MCV (fl) value in febrile seizure group was 69.5 (SD±5.90) and in control group it was 74.3 (SD±6.90) t test value was 6.36 and p<0.01. Mean MCH (pg) value in febrile seizure group was 22.3 (SD±3.20) and in control group it was 24.1 (SD±3.05) t test 4.98 p<0.01. Mean MCHC (gm/dl) value in febrile seizure group was 30.2 (SD±2.12) and in control group was 31.4 (SD±1.30) t test value was 5.91 p<0.01 (Table-1and Graph-1). In estimation of serum ferritin (mg/ml) the mean value in febrile seizure group was 40.8 (SD±19.2) and in control group it was 65.9 (SD±25.4) t test value 9.6 and p value was highly significant (p<0.01) (Table-2and Graph-2). These findings were more or less in agreement with previous studies11,12,13. Iron deficiency anaemia cases are reported in many studies in developing countries with the percentage being 44-66% of children under the age of 4 years14.Iron deficiency interferes with the function of many organs leading to anaemia, abnormal growth and behaviour, cognitive deficits, altered thermoregulation, impaired physical performance and immune dysfunction. Iron is important for catecholamine metabolism and for the various enzymes and neurotransmitters present in central nervous system. It increases extra cellular dopamine and norepinephrine levels in the caudate – putamen nucleus and decreases the levels of dopamine D1and D2 receptors and monoamine transmitters. Furthermore, iron deficiency in early life alters metabolism and neurotransmission in major brain structures such as basal ganglia and hippocampus and disrupts myelination. Iron deficiency is associated with several neurological disorders such as restless leg syndrome breath holding spells and attention deficit hyperactivity disorders which are associated with increased brain excitability. ID leads to febrile seizure was also experimented in mice 15 and were more prone to infection too.
SUMMARY AND CONCLUSION The present study suggests that IDA can serve as important influencing factor for the febrile seizures in children. Thus, IDA can be added to the list of risk factors for the FS. This study demands further patho-physiological, nutritional, genetic and pharmacological studies to know the exact mechanism or relation of IDA to FS. This research paper was approved by Ethical Committee of Sardar Patel Medical College, Bikaner (Rajasthan) Table 1: Comparison of haematological profile in both groups
Graph 1: Comparison of haematological profile
Table 2: Comparative study of serum ferritin in both groups
Graph 2: Comparative study of serum ferritin in both groups
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.