 Home
Home
|
Table of Content - Volume 18 Issue 2 - May 2021
Association of body composition with severity of asthma
K Rugmini1, K Divya2*, K E Elizabeth3, Sanjay Masaraddi4
1Professor, 2Junior Resident, 3Professor & HOD, 4Associate Professor, Department of Pediatrics, Sree Mookambika Institute of Medical Science, Kulasekharam, Kanyakumari District, Tamil Nadu-629161, INDIA. Email: drdivyarao.15@gmail.com
Abstract Background: The prevalence of asthma is up to 23% among Indian children. Obesity and under nutrition is known to have an effect on asthma. Objectives: To study the association of nutritional parameters-Weight for Age (WFA), Height for Age (HFA), Body Mass Index (BMI), Body Fat Percentage (BFP), Lean Body Mass (LBM) and Fat Free Mass Index (FFMI) on severity of asthma. Settings and Design: This was a cross-sectional study, conducted in the department of Paediatrics of a teaching hospital from April 2018-May 2019. Materials and Methods: 40 consecutive 5-15 year-old-children with clinical diagnosis of asthma were included in this study. Severity of asthma was categorized according to GINA Guidelines 2018-Well controlled, Poorly controlled and Uncontrolled. Weight, Height and BMI were recorded. BFP and LBM were estimated using Deurenberg formula and Boer’s equation respectively and FFMI was derived from fat free body mass and height. Statistical Analysis: Statistical analysis was done using SPSS software version 16.0 and the association between asthma and nutritional parameters were analyzed by Chi-square test. Group comparison was done using one-way ANOVA test. Observations and Results: Out of 40 children, 7 (17.5%) were underweight and 6 (15%) stunted. 3 (7.5%) were obese and 2 (5%) were overweight. Male female ratio was 1.5:1. There was a significant negative association between nutritional status and severity of asthma; WFA (p-0.002), HFA (p-0.015), BMI (p-0.000), BFP (p-0.031), LBM (p-0.000) and FFMI (p-0.000). Conclusion: In the study, underweight and stunting indicating under nutrition was more than overweight and obesity. All the nutritional parameters, WFA, BMI, BFP, LBM and FFMI showed significant negative association with severity of asthma (p<0.05). Periodic monitoring of nutritional status and appropriate nutritional intervention to reduce the severity of asthma is recommended as there was significant association between under nutrition and severity of asthma. Keywords: BMI, Body Fat Percentage, Fat Free Mass Index, Lean Body Mass, Nutritional status, Severity of asthma.
INTRODUCTION Asthma is a common cause of morbidity and preventable mortality. The proportion of Indian school children suffering from Bronchial Asthma has increased to more than double in the last 10 years reaching a prevalence of up to 23%.1 It was observed by Cohen et al., that there was an association between asthma and growth inhibition, and that the persistence of allergic symptoms caused retardation in stature and bone maturation.2 It is also known that loss of body mass produces disturbances in breathing physiology; diminution of diffusion capacity and increased air-trapping occur as a consequence of dyspnea and vice versa.3 Early onset of disease may contribute for growth retardation.4 Children with asthma may get recurrent attacks and hospitalizations, and there is a chance that they can go for under nutrition. This in turn can reduce the muscle mass and can increase the severity of asthma. Treatment with corticosteroids may reduce the final growth. Hence it is important to assess the nutritional status in these children. The Body Fat Percentage (BFP) is a measure of fitness level which directly calculates a person's relative body composition without regard to height or weight. BFP shows good correlation with BMI (Body Mass Index). BFP can be estimated from the BMI by using formulae derived by Deurenberg (1.51 x (BMI) .70 x (age - 3.6) x (sex + 1.4) where males=1, females=0].5 Lean Body Mass (LBM) is a component of body composition which is obtained by subtracting body fat weight from total body weight. LBM has been described as an index superior to total body weight, for prescribing more accurate levels of medications and also for assessing metabolic disorders, as body fat is less relevant for metabolism. It can be derived from simple techniques such as waist circumference, skin fold thickness or more accurately by using Dual Energy X-ray Absorptiometry. Yet another method is by using Boer’s equation (0.407W + 0.267H − 19.2 (kg) for boys and 0.252W + 0.473H − 48.3 (kg) for girls).6 Fat free mass (FFM) refers to the mass of metabolically active organs [7]. Fat Free Mass Index (FFMI) is a formula that calculates the amount of muscle mass a person has in relation to his or her height. It is a relationship between fat free mass (lean mass) and height. FFMI is considered to be a prognostic marker and a superior method of calculating a person’s body condition and health. It is derived by formula, FFMI=Fat free mass in (kg) x height -2(m).
MATERIALS AND METHOD 40 consecutive children aged 5 to 15 years with clinical diagnosis of asthma attending Paediatric Out Patient Department in a tertiary care centre were included in this cross sectional study conducted from April 2018-May 2019. Inclusion Criteria: Children in the age group 5-15 years diagnosed with asthma, and who attended our OP during the study period and gave consent for this study Exclusion criteria: Those who had other morbidities like Congenital Heart Disease, Cystic Fibrosis, CNS abnormalities, Endocrine or Hematological abnormalities and Congenital Malformations were excluded. Classification of patients with Asthma: According to GINA Guidelines 2018, asthma symptom control was categorized into 3 subgroups as I)Well controlled, II)Poorly controlled and III)Uncontrolled; based on day and night symptoms, reliever used and activity limitation for the past 4 weeks and FEV1.FEV1 was assessed for all children using CareFusion Spirometer, which uses Spirometry PC Software (SPCS). Risk factors for poor asthma outcomes were also taken into consideration. Study Parameters: Weight, Height and BMI were recorded in all children.Body weight was measured on a Phoenix calibrated balance to the nearest 0.1 kg. Height was measured to the nearest 0.5 cm while patients were barefoot and standing with their backs and heels touching a vertical bar. BMI was calculated from this data using the formula BMI= weight (kg)/height (m2). BFP was estimated using Body Fat Percentage formula [1.51 x (BMI) .70 x (age - 3.6) x (sex + 1.4) where males=1, females=0].5 LBM using Boer’s equation [0.407W + 0.267H − 19.2 (kg) for boys and 0.252W + 0.473H − 48.3 (kg) for girls] [6], FFMI using the formula, FFMI= [Fat free mass in (kg) x height-2 (m)].7 Ethics: Institutional ethics committee approval, Informed consent from parents and assent from children >7 years were taken, prior to enrolment. Statistical Method: Analysis of data was done using SPSS version 16.0. Association between WFA, HFA, BMI, BFP, LBM and FFMI and severity of asthma were analysed by Chi Square test. Group comparison was done using one-way ANOVA test.
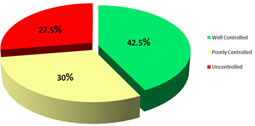
OBSERVATIONS AND RESULTS Out of 40 children, 24 were males and 16 were females (ratio-1.5:1). 16 were in the age group 5-10 years and 24 were in the age group 11-15 years. All of them belonged to socioeconomic status of Upper and Lower Middle Class. Out of 40 children, 7 (17.5%) were underweight and 6 (15%) stunted. 3 (7.5%) were obese and 2 (5%) were overweight according to India Academy of Paediatrics growth charts 2015. Among the 40 children, 17 (42.5%) had well controlled, 12 (30%) poorly controlled and 11 (27.5%) had uncontrolled asthma (Figure 1). Figure 1: Classification of Severity of Asthma
Mean WFA of the total group was 96.89 % but those who had poorly controlled asthma had a mean WFA of 81.42 % whereas it was 108.85% in the subgroup of Well controlled asthma. BMI of the subgroup of Uncontrolled asthma was only 14.76, whereas in the Well controlled subgroup it was 20.40. Mean BFP of the total group was 18.51%, with a mean of 15.17% in Uncontrolled, 17.09% in Poorly controlled and 21.10% in Well controlled subgroups. The mean LBM of the group was 29.60 Kg, but those in Uncontrolled subgroup had a mean of only 21.05 Kg. Mean FFMI was 14.95, 12.63, 14.51 and 16.7 for the total group, Uncontrolled, Poorly controlled and Well controlled subgroups respectively. HFA was almost as same in all the three subgroups. Severity of asthma was found to be increasing with a decrease in all the anthropometric parameters assessed above like WFA, BMI, LBM and FFMI as evidenced by a significant negative association with severity of asthma (p value <0.005). But for HFA and BFP the negative association was significant but to a lesser extent (p value <0.05) (Table 2).
Table 2: Association of Nutritional Parameters with Severity of Asthma
*Significant p value <0.05
DISCUSSION This study was an attempt to find the impact of nutritional parameters on asthma severity. It is a known fact that obesity is a risk factor for asthma. Under nutrition and its association with asthma is less studied and those studies which are done gave varying results. In our study, majority of children belonged to well controlled asthma category. There was almost an equal prevalence of severe asthma and moderate asthma in the study population which can be attributed to the fact that the study was done in a referral centre. Majority of children had under nutrition but 12.5% children were overweight/ obese. Still there was a significant negative association between WFA, BMI and severity of asthma. This shows the overwhelming effect of under nutrition (increasing the severity of asthma) in the study group. Way back in 1940, itself Cohen et al. observed that if asthma symptoms persisted it compromised height and bone maturity.2Similar to our study, Falliers et al., observed that children with severe asthma had height below normal.8Mc Nicol also observed that there is a negative correlation between height and severity of asthma.9 But in our study the mean height was almost equal in all the three subgroups and a group comparison of HFA and severity of asthma showed a negative association but with a p value of 0.015(<0.05). A previous study by Marcinello et al., showed that asthmatic children had significantly less weight and height but not BMI than their non asthmatic peers10 in contrast to our study which showed a significant association between BMI and severity of asthma (p=0.000). A study done by Reyes M et al., showed that asthmatic children who were mild and moderately malnourished had high levels of specific IgE.11 and this can be taken as indirect marker for atopy or asthma. All these studies are in concordance with our finding suggesting that underweight has a significant association with the severity of asthma. A causal relationship between severity of asthma and under nutrition cannot be established, as significant morbidity, hospital visits and financial burden on the family may be a contributing factor for under nutrition in these children. In contrast to all these a large study done in Brazil concluded that there was no association between nutritional status and severity of asthma.12Among the derived parameters those measuring the muscle mass (LBM and FFMI) showed a very strong association with the severity of asthma showing a p value of 0.000. BFP showed a significant negative association with severity of asthma (p value 0.031) but not as significant as LBM and FFMI which had a p value of 0.000. It can be inferred that decreased muscle mass has a major role in determining the severity of Asthma than the fat percentage but this needs further studies to confirm. Collaborative evidence for this is Marcelino’s study where decrease in respiratory muscle strength was seen especially in patients with severe asthma.10 Moreover, a study done by Stojanovic et al., in adults showed that malnutrition has a major role in asthma and that lower percentage of muscle mass was associated with more exacerbations and low FFMI with obstruction in asthma‑.13 These results can be extrapolated in children. A previous study done by Wang R et al., showed that increase in Body Fat Percentage was associated with reduced FEV1 and FVC in boys even though increase in BMI was associated with an increase FEV1 in girls,14 but in this study girls were less in number necessitating further study to confirm.
CONCLUSION In the study more children were under nourished. However, 12.5% were over nourished. Anthropometry as a reflection of nutritional status has got a negative association with severity of asthma. Fat Free Mass Index was found to have major effect on increasing the severity of asthma than Body Fat Percentage. It is recommended that reduced muscle mass leading to decreasing mass and strength of respiratory muscle fibres needs proper nutritional corrective measures. This study recommends periodic monitoring of nutritional parameters and appropriate intervention in children with asthma. Supplementing and correcting nutritional status may improve the muscle mass which may in fact reduce the severity of asthma.
LIMITATIONS Variable and Low sample size in the study. All parameters were calculated using formulas- techniques like Dual Energy. X-ray Absorptiometry (DEXA) or Bioelectrical Impedance Analysis was not used. Reassessment after nutritional management in the same study group was not undertaken. The effect of steroid prophylaxis on the nutritional status needs further studies.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.