 Home
Home
|
Table of Content - Volume 21 Issue 1 - January 2022
Jarcho levin syndrome: A case report
Aromita Deb1*, Ghazi Sharique Ahmad2, Santosh Kumar3, Md Habibul4, Gupta Bhushan Devendrakumar5
1,4,5Post Graduate Trainee, 2Professor & HOD, 3Associate Professor, Department of Pediatrics, Katihar Medical College, Katihar, INDIA. Email: msaromitadeb@gmail.com
Abstract Jarcho Levin Syndrome is a congenital disorder characterised by the presence of ribs and vertebral defects right from the birth. These present multiple vertebral anomalies at different levels of the spine including “butterfly vertebrae” hemivertebrae and fused hypoplastic vertebrae. It can also lead to respiratory compromise and death in infancy in certain individuals due to the small size of thorax. Here we report a new case who is a 11 years old female with swelling over the chest which was progressive in nature, short neck and respiratory problems on lying down. Key Word: Jarcho levin syndrome.
INTRODUCTION Jarcho Levin syndrome is a rare genetic disorder characterized by defects of the bones of the spines (vertebrae) and abnormalities of the ribs. Ribs are missing or fused in chaotic patterns. These malformations are present from birth (congenital) Is inherited in an autosomal recessive manner and is caused by a change in mutation in one of the following four genes: DLL3, MESP2, LFNG, HES7. There are two subtypes: Spondylothoracic dysostosis and Spondylocostal dysostosis, The signs and symptoms can vary from one person to another, the small size of the thorax in newborns frequently leads to respiratory compromise and death in infancy. some variants with survival into adulthood have also been described. It is primarily characterized by a short neck, short trunk and a constricted thorax (narrow fetal thorax) due to multiple ribs (crab like or fan like radiation of the ribs) and vertebral anomalies at all levels including: Butterfly vertebrae. Hemivertebrae. Fused veterbrae. Hypoplastic vertebrae
CASE REPORT 11 years old girl presented to us with progressive swelling over the chest and difficulty in breathing on lying down. Born out of a non consangious marriage at a community hospital by vaginal delivery to a 20 year gravida 1 para 0 mother, it was a uneventful delivery, she cried immediately after birth, she has a small swelling over the chest right from the birth, but on intervention was taken on it. The mother was a unbooked case, had two antenatal visits, and had two antenatal ultrasonography done, she did not use alcohol, tobacco or illicit drugs during the pregnancy. She began walking at eight months old, at five years of age she was noted to have a disproportionately short neck, and the swelling over the chest progressively was increasing, but otherwise well developed, no limitation in daily activity. On examination: Short neck. Crab chest noted on the right side. Scoliosis noted. Anthropometry: Height for age: 125.2 cms (below 3rd centile for the age and sex). B.M.I: 13.7 (between 5th and 10th centile for the age and sex). No facial deformity. No other significant findings.
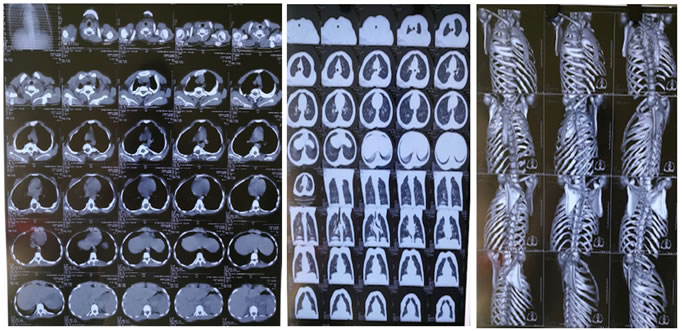
Imaging: NCCT thorax: Figure 1 Figure 2 Figure 3
There is fusion of left 1st, 2nd, 3rd, and 4rth ribs postetiorly, right 3rd, 4rth, 5th posterior ribs and right 3rd and 4rtg anterior rib with resultant crab like configuration. There is fusion of the posterior elements of D1 to D5 vertebrae with partial /near complete fusion of theor end plates. There is mild degrees of upper sternal protrusion anteriorly with concavity of right lateral border with asymmetrical chest wall. Posterior spina bifida seen at D5 and D6 levels. there is kyphoscoliotic deformity at the upper dorsal spines, concavity towards left. B/L lung fields appears normal and show attenuation pattern. Mediastinum is in midline. No evidence of pericardial/pleural effusion. Cardiothoracic ratio normal. IMPRESSION: multiple b/l ribs fusion /synostosis with upper thoracic vertebral anomalies and fusion. S/O: Jarcho Levin syndrome variant ( spondylo-costal variant).
DISCUSSION Jarcho Levin syndrome is a rare disorder. the exact prevalence and incidence is unknown. Affects both males and females equally, it is a autosomal recessive disorder, it occurs due to the change in mutation in one of the four genes: DLL3, MESP2, LFNG, HES7. The diagnosis is based upon identification of characteristic symptoms, a detailed patient and family history, a through clinical evaluation and a variety of specialized tests. The diagnosis can be confirmed through molecular genetic testing in some individuals. Prenatal diagnosis can be made through fetal ultrasound, genetic counselling in needed. Treatment may require coordinated efforts of a team of specialists, paediatricians, specialists who treat and diagnose skeletal disorders, orthopedic surgeons, cardiologist, pulmonologists and other health care professionals may need to systematically and comprehensively plan an affected Childs treatment. psychosocial support is needed for the whole family. Infants who experience some kind of breathing problem can require some form of respiratory support, may require intensive care which also involved constant monitoring in the hospital. If scoliosis is severe enough, surgery may be required to straighten the spine.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.