 Home
Home
|
Table of Content - Volume 18 Issue 1 - April 2021
Computed tomographic study in seizure disorder
Manoj Kumar1*, Dhara Mahendra2
1Consultant Radiologist, Jaipur, Rajasthan, INDIA. 2Associate Professor, Department of Ophthalmology, SMS Medical College, Jaipur, Rajasthan, INDIA. Email: drdharamanoj@gmail.com
Abstract Background: To study the CT scan characteristic in patient with seizure disorder and categorize the nature of lesion. Materials and methods: This study was conducted on 100 patients with seizure disorder came to Radiology department of SP Medical College Bikaner. Observations and Results: Analysis of cranial CT scan showed normal study in 45% of the cases and abnormalities in 55% of the cases. CT scan abnormalities were classified as infectious, post infectious, neoplastic, cerebrovascular disease, congenital lesions, traumatic lesions, post traumatic sequele, tubercular infection and neurocysticercosis. Seizure disorder is a common neurological disease with different aetiologies. Neuro imaging is important diagnostic and prognostic tool in evaluation of patient with seizure disorder. CT scan is often initial investigation in emergency situations. CT scan is cost effective diagnostic tool developing countries with limited resources. Conclusion: CT scan useful diagnostic modality in evaluation and management of patient of seizure disorder. Keywords: brain, cranial, CT scan, seizure.
INTRODUCTION Knowledge of etiopathogenesis of seizure disorder is of paramount importance in planning and executing effective treatment. In many cases however no lesion of any description could be demonstrated. Moreover, an organic lesion of brain of some nature may be associated with seizure in many cases. Improved investigation techniques like computed tomography (CT scan), magnetic resonance imaging (MRI), position emission tomography (PET), single photon omission computerized tomography (SPECT) and isotope brain scanning all have provided invaluable tools for detection and localisation of structural abnormalities of the brain in patients of seizure disorder. CT scan can provide a sensitive and reproducible method for evaluating suspected lesion in central nervous system. It is often the investigation of choice of evaluating the CNS lesion whether or not other modalities like MRI are available. CT scan system consists of three main components (1) Imaging system (2) scanning system (3) power cabinet. The majority of scanners in use at present are third-generation rotate only system. Classification of seizures
The likely etiology of given seizure depend on age of the patient and type of the seizure. In neonates’ common causes are perinatal hypoxia, ischemia, metabolic disturbance, developmental disorder, genetic disorder, trauma, acute CNS infection and intracranial haemorrhage. In infants and children of less than 12-year common causes are febrile seizure, CNS infections, development and genetic disorders and idiopathic. In adolescent between age of 12 - 18 years common causes are trauma, infections, genetic disorder, brain tumours, drug abuse and idiopathic. In young adults between age of 18 - 35-year causes are alcohol withdrawal, trauma, illicit drug use, brain tumour and idiopathic. In older adults more than 35 year of age causes are generally brain tumour, alcohol withdrawal, cerebrovascular disease, metabolic disorder, idiopathic, Alzheimer disease and other degenerative CNS disease. AIMS AND OBJECTIVES
MATERIALS AND METHODS This study was conducted on 100 patients with seizure disorder reporting to various emergency, inpatient and outpatient departments and referred to department of radiodiagnosis in Sarder Patel Medical College Bikaner. General particulars of the patient such as age, sex, residence, occupation, religion, drug history, dietary history was noted. The concerned referring clinician’s account of presenting complaint of each patient was documented. Further details of present and past history of illness were elucidated from the patient or attendant as per circumstances. Physical examination in general and CNS examination in particular was conducted. Results of all investigation which were undertaken were recorded particularly X ray skull, EEG report and various blood investigations. Following registration cranial computed tomographic evaluation of each patient presenting with seizure was done on SomaTom art, 3rd generation rotate type whole body CT scanner from Siemens and high speed NX/ 1 pro dual slice from GE which was installed in our hospital. Technique: The patient was kept in supine position with table position adjusted to individual need. The head was immobilized with in a special headrest with special head support. Facilities for proper immobilisation were provided and patient was given instruction to avoid any movement. Restless patients and children were sedated as required. First a sagittal planning topogram scanogram was acquired at low resolution. This image served to determine the desired scan angle and planes. The orbit m et al. lines were selected because these fixed points are readily defining the top of orbit and external auditory meatus. Then the axial CT sections of the entire cranial cavity and its content were taken. Generally, slice thickness of 10mm was selected. However, slice thickness was adjusted as per requirements. The gantry was tilted to an appropriate degree so as to obtain a plane of section of 15 -20 degree to canthomeatal line. Computer programs of magnification distance and density measurement and viewing at proper window level was utilised. Additional contrast-enhanced scan was performed as and when required by IV injection of appropriate dose of contrast medium after sensitivity testing. CT head findings were read as follows Soft tissue structure - any bruises or tumour. Quadrigeminal and basal cistern-normal or brain stem herniation. Size and contour of ventricles and subarachnoid space- Appropriate for the age of patient, any dilatation, obstructive /non–obstructive hydrocephalus. Any mid line shift of the structures. Periventricular white matter and cortex –insconspious and well-defined local lesion, local edema Basal ganglia, internal capsule, brainstem, pons, cerebellum. Calcification, focal/diffuse lesions, hypodense/ hyperdense, location, size, shape, number, margin, density. Surrounding tissue and enhancement pattern. Bony details- fracture, metastasis. Finally, the conclusion of CT findings was made. Table 1: Type of seizure distribution of 100 cases of seizure disorder
Seizure was classified in generalized, partial and unclassified on the basis of clinical feature most common seizure was generalized in 62% of cases and second was partial in 34% of cases.
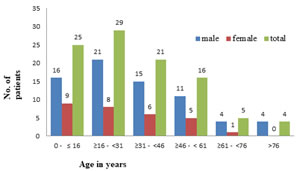
Table 2: Age and sex distribution of 100 cases of seizure disorder
Maximum number of patient with seizure 29% occurred in 16 to 31 years age group followed by 25% cases in less than 16 years age group. These two age group account for about 54 % of total patient. Male (71) are more commonly affected than females (29) in ratio of 2.45: 1. Chart 1: Age and sex distribution of 100 cases of seizure disorder
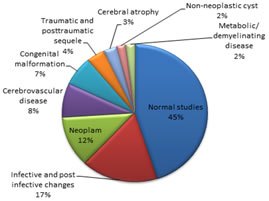
Table 3: CT findings in the study 100 patients of seizure disorder
In this study 100 patients with seizure, normal studies were found in 45 cases (45%). The majority of abnormal scans revealed infective and post infective changes found in 17 cases (17%.). Neoplasm were found in 12 cases, cerebrovascular disease in 8 cases, congenital malformation in 7 cases , traumatic and posttraumatic sequele in 4 cases, cerebral atrophy in 3 cases, non-neoplastic cyst in 2 cases, metabolic/ demyelinating disease in two cases.
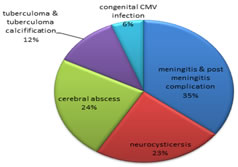
Chart 2: CT findings in the study 100 patients of seizure disorder Infective and post infective complication constituted the largest group of intracranial pathology and accounted for 17 cases out of 100 patients of seizure disorder. Meningitis and post meningitis in 6 cases, and neurocysticercosis 4 cases, cerebral abscess 4 cases, tuberculoma and post tuberculoma calcification in 2 cases, congenital CMV infection 1 case. Tuberculous infection was the most common infective pathology out of hundred seizure patients accounting for 6% including to tubercular meningitis and tuberculoma in our study population. NCC was the most common helmintic infection seen in 4% cases out of hundred cases.
Chart 3: Analysis of Infective and post infective changes
DISCUSSION The study was conducted in 100 patients with seizure order referred to department of Radio diagnosis at SP Medical College for computerized tomography scanning of head. Largest number of affected patient in this study belongs to 16 to 31 year of age group next belong 0 to 16 year age group. Male were affected with seizure more than females in ratio of 2.4: 1. Out of 100 seizure cases generalize seizure found in 62%, partial seizure in 34% of cases and rest included in unclassified type. Analysis of cranial CT scan revealed normal study in 45% of the cases. Structural abnormalities on CT scan were found in 55% of cases. An attempt was made to identify the nature of lesion on basis of CT scan characteristic to arrive at a definitive diagnosis and facilitate treatment. CT Scan abnormalities were observed in 55% of the patient and classified as infectious and post infectious in 17%, neoplastic in 12%, cerebrovascular disease in 8%, congenital lesion in 7%, traumatic lesion and post traumatic sequel found in 4%, cerebral atrophy in 3% and miscellaneous group including non-neoplastic cyst in 2% and demyelinating and metabolic disease in 2%. Infective and post infective complication constituted the largest group of intracranial pathology and accounted for 17% (17 cases) includes meningitis and post meningitis in 6%, neurocysticercosis in 4%, cerebral abscess 4%, tuberculoma and post tuberculoma calcification in 2%, congenital CMV infection in 1% of cases. This study concluded that CT could be cost-effective alternative to MRI in suspected cases of NCC in single episode of seizure especially in endemic region like part of India because of high sensitivity of C T for calcification. Neoplasm comprise the second largest group of lesion accounting for 12% cases, of which meningioma and astrocytoma constitutes more than 50% of the cases and 25% was secondaries. 41.6 % of the neoplasm presented with chronic seizure and observed that CT head is valuable tool in discovering potentially removable lesion in chronic epileptic patients. Cerebrovascular disease emerged as third most important cause with 8% cases. Infarction constitutes more than 50% of CVA lesions associated with seizure disorder. In present study post infract seizure observed more commonly when temporal cortex was affected area. Congenital lesion were found in 7% of cases including cyst of CSP and CV, cyst of CVI, schiezoencephaly and dandy Walker malformation, corpus callosum agenesis and porencephalic cyst. Traumatic lesion and posttraumatic sequele were found in 4% of the cases. Majority of the patient presented with multiple traumatic lesions. Two cases of the non-neoplastic cyst were found including arachnoid and colloid cyst one each. Two case of the metabolic and demyelinating disease were found including FHAR disease and ADEM. In present study three cases were found of cerebral atrophy in which two cases were diffuse cerebral atrophy and one case of cerebral hemi atrophy. Two cases came with seizure and cerebral palsy. One case had cerebral atrophy and second had corpus callosum agenesis on CT scan. These were comparable with previous literature. The finding observed that static and developmental lesion is as common as infection in our study because of selection population is in developing country where infection is very common.
CONCLUSION Cranial CT scan is a useful investigation procedure in patient with seizure disorder. Structural abnormalities on CT scan can be defined on the basis of type and site of pathology in brain in patient with seizure. CT scan characteristic of lesion helps in accurate diagnosis of seizure disorder. CT scan often is initial investigation in emergency situation when other modalities are not available. So CT scan is a choice of modality in country like India with limited facility of advance modality to scan.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.