 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 3 Issue 1 - July 2017
A Horseshoe Kidney: A Case Report
R R Bokan1*, K Shyamkishore2
1Resident, Department of Anatomy B.J.G.M.C. Pune, Maharashtra, INDIA. 2Associate, Professor Department of Anatomy Seth G.S.M.C. Mumbai, Maharashtra, INDIA. Email: rajubokan@gmail.com
Abstract During abdominal dissection carried out in the Department of Anatomy, Seth G.S.M.C. KEMH Parel, and Mumbai a horseshoe kidney was observed in 40-year-old male cadaver. The kidney was placed at lower position as compared to its normal position. The lower pole fused to form the isthmus against L4 vertebra. Relation of structures in hilum pelvis was anterior to vein and artery on both sides. The right and left renal arteries arose as lateral branches of the aorta just below the level of superior mesenteric artery. One accessory renal artery originated from the ventral aspect of aorta just above the isthmus. Right kidney was drained by 3 renal veins while the left kidney was drained by a 2 renal veins into IVC. Embryological basis and clinical significance of such anomaly is very important in planning and conducting surgeries. Keywords: Accessory renal artery, anomalous kidney, Horseshoe kidney.
INTRODUCTION Horseshoe kidney is a known congenital anomaly of the upper urinary tract. The frequency of appearance is 1/400–8001. In the horseshoe kidney there is a fusion of the lower poles or upper pole of both kidneys. During migration from the sacral region the two metanephric blastemes can come into contact at the more commonly at the lower pole. The bridge of parenchyma by which they are joined is called the isthmus. When the isthmus of a horseshoe kidney reaches the level of origin of inferior mesenteric artery from the aorta, it cannot rise further. This leads to arrest of ascent at L3 level.
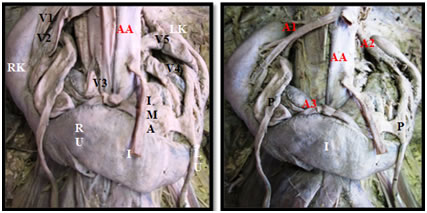
OBSERVATION AND RESULT During a routine abdominal dissection carried out in the Department of Anatomy, Seth G.S.Medical College and KEM Hospital Parel, Mumbai a horseshoe kidney (U-horseshoe) was observed in 40-year-old male cadaver. The kidney was placed at ectopic position as compared to its normal position. The lower poles were fused to form the isthmus(I) opposite to the L4 vertebra. There was no extra renal anomaly. Relation of structures in hilum pelvis was anterior to vein and artery on both sides. The right and left renal arteries (A1 and A2) arose as usual as lateral branches of the aorta just below the level of superior mesenteric artery. One accessory renal artery (A3) originated from the ventral aspect of aorta just above the isthmus. Right kidney was drained by three renal veins (V1, V2 and V3) directly into the inferior vena cava while the left kidney was drained by a two renal veins (V4 and V5).
Photograph (1) Photograph (2) Photograph (1): RK:-Right kidney, LK: - Left kidney, RU:-Right ureter, LU:-Left ureter I: - Isthmus IMA:- Inferior mesenteric artery ,V1, V2 and V3 Renal veins, AA:-Abdominal aorta. Photograph (2): A1, A2 and A3:-Renal arteries, P:-Pelvis, IMA:-Inferior mesenteric artery, AA:-Abdominal aorta. DISCUSSION Horseshoe kidney can be U-horseshoe or L-shaped. The morphologic appearance related with the manner of fusion. Fusion on the midline results symmetric horseshoe Lateral fusion, an asymmetric kidney isthmus lateral to the midline, and crossed renal ectopia2. In present case, symmetrical fusion of the kidneys was observed. Isthmus ventral to the abdominal aorta and midline. Horseshoe kidney is located in a lower lumbar region at the L3-L5 vertebral level In front of the aorta and IVC Posterior to the inferior mesenteric artery, which usually crosses isthmus3. In present case, the right kidney situated between the L2- L3 to the L5 vertebra corpus. The left kidney was situated between L1 -L2 to the L4 vertebra. Associated with other anomalies, not in present case. Oktem H et al study shows in their case there were two arteries on the right side supplying blood to the two kidneys. The third one (A3) directly arose from the aorta above the origin of the IMA and supplied the isthmus and venous drainage of both kidneys and the isthmus were taken by three veins that opened independently into the IVC4. In present case the right and left renal arteries arose as usual as lateral branches of the aorta just below the level of superior mesenteric artery. One accessory renal artery originated from the ventral aspect of aorta just above the isthmus. Right kidney was drained by three renal veins directly into the inferior vena cava while the left kidney was drained by a two renal vein. Embryological basis Horseshoe kidneys results from an embryological malformation develops between the 4th and 8th week of intrauterine life. Metanephric blastemes become fused before rotation and migration. Fusion prevents independent rotation .Vessels thus develop an abnormal relation to the renal pelvis and ureters. During ascent of kidneys, they pass through the fork of umbilical arteries. Fork pushes renal blastemes so close that lower poles get fused. The normal kidney ascents from the sacral to the lumbar region. Horseshoe kidneys are ectopic. Sited at the root of IMA from the abdominal aorta. Ascent of kidneys arrested because isthmus get trapped beneath the IMA. Kidney rotation arrested, so the hilum of kidney faces ventrally. Ureter passes ventral to the isthmus of kidney. Change in location result from disproportionate growth of embryo caudal to the metanephros3. Horseshoe kidney is sometimes associated with Turner's Syndrome (occurring in as many as 7%), trisomy 18 and trisomy 9. It occurs more commonly in patients with Trisomy 18, and neural tube defects. 1/3rd of patients with horseshoe kidneys have other abnormalities including those of the genito-urinary, gastrointestinal, respiratory, and skeletal systems. Malignancies like Wilms' tumor (the relative risks of each tumor are increased fourfold), Transitional cell carcinoma (the relative risks of each tumor are increased two fold), Carcinoid tumor (the relative risks of each tumor are increased 62 fold) 5. Clinical Significance Infection, Nephrolithiasis, Hydronephrosis or hydroureter secondary to narrowing or pelviureteral stenosis of ureter where it crosses isthmus, renal stone formation, Accessory renal arteries and Ureter can get angulated.
CONCLUSION Embryological basis and clinical significance of this congenital anomaly is very important for the radiologist and the surgeon to know the anatomical variations in the blood supply of horseshoe kidney as the surgery could be complicated in the presence of anomalous blood supply.
ACKNOWLEDGEMENT Dean, Seth GS Medical College and KEM Hospital Parel, Mumbai and Department of Anatomy, Seth G. S. Medical College and KEM Hospital, Parel, Mumbai
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.