 Home
Home|
Table of Content Volume 3 Issue 1 - July 2017
Hepatic artery variations studied on cadavers and its relevance in medical practice
Mane Uddhav Wamanrao1, Sunil J Pundge2*, Deepak S Joshi3
1Assistant Professor, Department of Anatomy, Dr. Shankarrao Chavan Government Medical College Nanded, Maharashtra, INDIA. 2Assistant Professor, 3Professor and HOD, Department of Anatomy, Grant Government Medical College and Sir JJ Group Of Hospitals, Byculla, Mumbai, Maharashtra, INDIA. Email: sunilpundge@gmail.com
Abstract Anatomical variations of Hepatic artery are known to occur in 25-50% of the total population. Deviations of the normal hepatic arterial pattern are not rare. Knowledge of these variations play clinically significant role in surgical and radiological interventional procedures. The variations in the hepatic arterial pattern were studied with meticulous dissection and observation, on total 60 adult embalmed cadavers of both sexes. Normal Hepatic arterial pattern was observed in 50 cadavers. Accessory right hepatic artery originating from the superior mesenteric artery in 5 cadavers and it was the most common variation. Other variation found was replaced or accessory left hepatic artery arising from the left gastric artery in 4 cadavers and right and left accessory hepatic arteries arising from the superior mesenteric and left gastric arteries respectively in 1 cadaver. Key Words: Hepatic artery, Common Hepatic artery, Proper Hepatic artery, left gastric artery, Accessory Right Hepatic artery, Accessory Left Hepatic artery, Superior Mesenteric artery, Celiac Trunk.
INTRODUCTION Anatomical variations of Hepatic artery are reported to occur in 25-50% of the total population1. The common hepatic artery arises from coeliac trunk along with splenic and left gastric arteries. It gives rise to the right gastric artery, gastro duodenal artery and continues as proper hepatic artery. The proper hepatic artery reaches the porta hepatis through the right free margin of the lesser omentum. In the lesser omentum the artery is anterior to the portal vein and to the left of bile duct. The hepatic artery proper gives a right gastric artery and then divides into right and left branches which supply the left and right lobes of the liver respectively. The right hepatic artery gives a cystic branch which supplies the gall bladder. Deviations of the above-described normal arterial pattern are not rare. Jonathan R. Hiatt et al2 described Hepatic arterial pattern in 1000 cases. He noted normal Arterial patterns in 75.7% (common hepatic artery arising from the celiac axis then it gives gastroduodenal and proper hepatic arteries, proper hepatic dividing distally into right and left branches). He described replaced or accessory right hepatic artery originating from the superior mesenteric artery, replaced or accessory left hepatic artery arising from the left gastric artery, both right and left hepatic arteries arising from the superior mesenteric and left gastric arteries respectively, entire common hepatic artery arising as a branch of the superior mesenteric artery and common hepatic artery originating directly from abdominal aorta. Knowledge of these variations play clinically significant role in hepatobiliary transplantation, resection, tumour embolisation as well as in extrahepatic abdominal surgeries involving the stomach, pancreas or gall bladder3. Knowledge of anatomical variations of the arterial pattern of the common hepatic artery is also important because it may influence interventional radiological procedures4,5.
MATERIAL AND METHODS The variations in the hepatic arterial pattern were studied with meticulous dissection and observation, on total 60 adult embalmed cadavers of both sexes allotted to undergraduate students in the Department of Anatomy, over the period of six years. Embalmed cadavers were procured from department of anatomy, government medical college with prior permission. Cadavers with intra-abdominal pathology that was interfering with the dissection were excluded. Each cadaver was dissected according to guidelines of Cunningham‘s manual of practical anatomy. Anterior abdominal wall was incised and musculocutaneous flaps were reflected laterally. Peritoneal cavity and the lesser sac were opened and branches of celiac trunk were identified. Then as dissection preceded, Common Hepatic Artery, Splenic Artery and Left Gastric Artery dissected carefully. All branches of these arteries were dissected finely. Lastly Superior Mesenteric Artery and Abdominal Aorta were dissected. Normal pattern and different variations were noted and photographs were taken. RESULTS We observed normal Hepatic arterial pattern (that is common hepatic artery arising from the celiac axis then it gives gastroduodenal and proper hepatic arteries, proper hepatic dividing distally into right and left branches) in 50 cadavers. We found accessory right hepatic artery originating from the superior mesenteric artery in 5 cadavers. We got replaced or accessory left hepatic artery arising from the left gastric artery in 4 cadavers. We observed right and left accessory hepatic arteries arising from the superior mesenteric and left gastric arteries respectively in 1 cadaver.
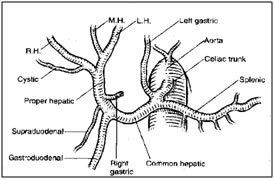
Figure 1 
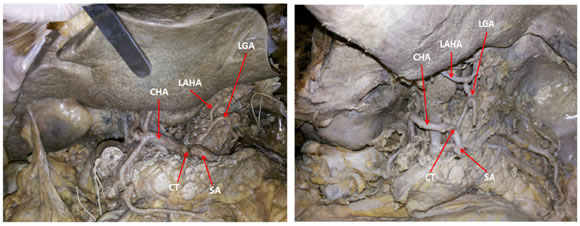
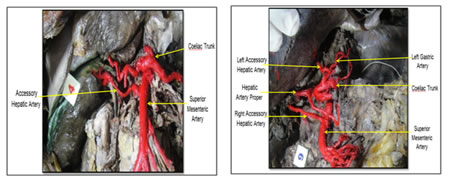
Figure 2 Figure 3 Figure 4 Figure 5 Figure 6 Figure 7 Legend Figure 1: Normal pattern of hepatic vasculature (RH, MH, LH Right, Middle, and Left Hepatic artery) Figure 2: Showing Left accessory hepatic artery (LAHA), Common hepatic artery (CHA), Left gastric artery (LGA) and Celiac trunk (CT). Figure 3: Showing Left accessory hepatic artery (LAHA), Common hepatic artery (CHA), Left gastric artery (LGA) and Celiac trunk (CT). Figure 4: Showing left accessory hepatic artery (LAHA), common hepatic artery (CHA), left gastric artery (LGA), celiac trunk (CT) and splenic artery (SA). Figure 5: Showing left accessory hepatic artery (LAHA), common hepatic artery (CHA), left gastric artery (LGA), celiac trunk (CT) and splenic artery (SA). Figure 6: Showing accessory hepatic artery arising from superior mesenteric artery. Figure 7: Showing right accessory hepatic artery arising from superior mesenteric artery and left accessory hepatic artery arising from left gastric artery. Knowledge of hepatic vascular anatomy is of great importance for the surgeon to perform abdominal intervention. It is known that changes present at different stages of embryonic development lead to large variations in vasculature Michels'6 classic autopsy series of 200 dissections, published in 1966, defined the basic anatomic variations in hepatic arterial supply. Variant patterns occurred in 45% of cases, and arteries could be defined as accessory or replaced because dissection was carried into the liver substance. He described normal hepatic vascular pattern in 55% cadavers, replaced left hepatic artery from left gastric artery in 10% cadavers, replaced right hepatic artery from superior mesenteric artery in 11% cadavers, accessory right and left hepatic arteries in 1% cadavers. Jonathan R. Hiatt et al2 study described normal hepatic vascular pattern in 75.7% cases, replaced or accessory left hepatic artery from left gastric artery in 9.7% cases, replaced or accessory right hepatic artery from superior mesenteric artery in 10.6% cases, accessory right and left hepatic arteries in 2.3% cases. Olival Cirilo Lucena da FONSECA-NETO et al7 study reported normal hepatic vascular pattern in 86.8% cases, replaced or accessory left hepatic artery from left gastric artery in 2.7% cases, replaced or accessory right hepatic artery from superior mesenteric artery in 5.6% cases, right hepatic artery arising from the superior mesenteric artery associated with the left hepatic artery arising from the left gastric artery 0.83%. The patterns of the hepatic vasculature among different studies are demonstrated in Table no.2. The findings of our study are consistent with the findings of the studies by Olival’s Study, Jonathan’s et al, Michel’s et al. Sarika rachel tigga et al8 reported an accessory hepatic artery emerging from the superior mesenteric artery to the right hepatic lobe. Srinivasarao Yalakurthy et al9 reported an accessory right hepatic artery arising from superior mesenteric artery which supplied the right lobe of the liver along with normal right hepatic artery same finding as our study. Katherine E Kondratuk et al10 reported replaced right hepatic artery, which originated from the SMA and coursed posterior to the portal vein and gave rise to the cystic artery in a cadaver during routine dissection. B.R. Chaitra and K.R. Dakshayani11 reported an accessory left hepatic artery was arising from left gastric artery and was entering the left lobe of liver comparable with findings of our study. Sukhendu Dutta and Bimalendu Mukerjee12 dissected 84 male cadavers and reported Normal hepatic arterial anatomy in 95% cadavers while 5% had accessory hepatic arteries.
Table 1: Distribution of patterns of hepatic vasculature
Table 2: Comparision of patterns of hepatic vasculature among different studies
CONCLUSION Detailed knowledge of hepatic arterial variations is of great importance to surgeons who perform approaches in this area. The left hepatic artery can provide accessory arteries that may be an important source of blood supply to the left lobe of liver. These variations presents as the potential bleeders during hepatobiliary surgeries and liver transplantation procedures. Preoperative knowledge of anomalous vessels is also helpful in modification of surgical approach. The origin of accessory hepatic artery from superior mesenteric artery is in close relationship with the head of the pancreas, first part of duodenum and the portal vein, makes it vulnerable during surgeries in this area. Kipping in mind these variations are useful for the planning and conducting of radiological and surgical procedures.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.