 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 1 -January 2018
Comparison of Propofol and Thiopentone as anaesthetic agents for electroconvulsive therapy - A prospective, double blinded cross over trial
Anand B*, Nimi G**, Selvakumaran***
*Professor, **Postgraduate Student, ***Assistant Professor, Department of Anaesthesiology and Critical Medicine, Meenakshi Medical College and Research Institute, Enathur, Kanchipuram – 631552, Tamil Nadu, INDIA. Email: cheetoo26@gmail.com
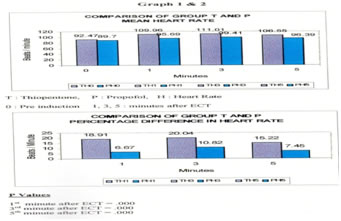
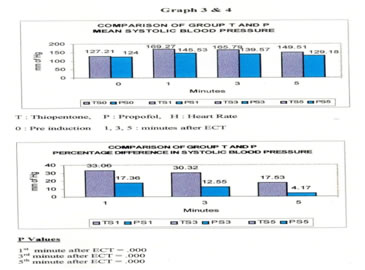
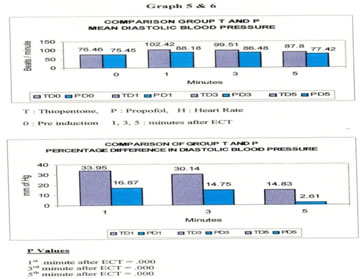
Abstract Background: The ideal anaesthetic agent for electroconvulsive therapy (ECT) should provide a smooth, rapid induction and recovery with minimal antagonistic effect on the seizure activity. We compared two induction agents- Propofol and Thiopentone for their effects on hemodynamic response, seizure duration and recovery characteristics during ECT. Method: We conducted a double blinded randomized repeated measure cross over trial in 50 patients planned for ECT under General Anaesthesia. Each patient received four sittings of ECT and the induction agent was alternated in each sitting. The main aim was to compare the duration of seizure activity, recovery time, hemodynamic parameters measured prior to induction and at various intervals after the conclusion of ECT among the two group: Group P (Propofol) and Group T (Thiopentone). Results: Maximal increase in Heart rate for both the groups, Group T(111.01/min ±17.62) and Group P (99.41/min ±16.97) was in the third minute with a higher increase in Group T. Peak Systolic blood pressure for both the groups was seen at the 3 mins, with a significant increase in Group T(165.79 mmHg ±23.87) than Group P(139.57 mmHg ± 16.28). Group T had a higher diastolic blood pressure (102.42 mmHg ±20.24) in the first minute when compared to Group P ( 88.18mmHg ±15.52) which also exhibited maximal increase in the diastolic blood pressure in the first minute. The seizure duration was shorter in Group P (19.65seconds ± 8.46) than Group T (27.98 seconds ± 10.97) seconds. Patients of Group T had a longer recovery time (10.39min±5.74) than Group P (7min±1.87). Conclusion: Propofol has better hemodynamic response with early recovery than Thiopentone and can be safely concluded as an ideal anaesthetic agent for ECT despite its effect on the seizure duration. Key Words: Propofol, Thiopentone, ECT, seizure, ideal anaesthetic agent.
Electroconvulsive Therapy (ECT) still retains a place in modern psychiatric practice as it is the mainstay of treatment in patients presenting with medication resistant depressive disorder, catatonia and mania. Anaesthetic agents are routinely used to modify convulsions produced by ECT1,2. The ideal anaesthetic agent for ECT should provide a smooth and rapid induction and recovery. It should cause attenuation of physiological effects and should have minimal or no antagonistic effect at all on seizure activity. It is therefore important in the selection of anaesthetic agents for ECT to consider the side effect profile of the drug on the response to the brain to the administration of the electrical current. The latter area includes consideration of variables like the duration of the seizure, degree of hypertensive response during the seizure, neuroendocrine responses and any other changes in brain physiology. The anaesthetic induction agent, Propofol has many pharmacological properties that makes it suitable for this purpose3. It produces less nausea and obtunds the hypertensive response that occurs with ECT more effectively than Thiopentone4 without causing undue hypotension. Initial concerns that shorter seizures produced with propofol administration may compromise efficacy have not been empirically supported in the period immediately after ECT and have been offset by its demonstrated advantages. Thiopentone was being used till date for all ECTs despite its side effects like prolonged wakening time, arrhythmias and laryngeal spasm. The aim of this study is to compare Propofol with Thiopentone for their effects on haemodynamic response, seizure duration and recovery characteristics during ECT.
MATERIALS AND METHOD This study was conducted in Meenakshi Medical College and Research Institute in the Department of Anaesthesia in co-ordination with the Department of Psychiatry during the period 2003-2009. The college ethical committee approval was obtained. 50 patients belonging to ASA class I (48) and II (2) were included consisting of 22 females and 28 males. The age of the patients varied between 18 to 65 years and the mean age was 33.56 years. All uncooperative patients were excluded. The study design was a double blinded randomized repeated measure cross over trial. All patients gave complete history and were physically examined before the ECT. Investigations were done as for the routine conduct of general anaesthesia including ECG and Chest X-ray. ECT was carried out in the morning with patient fasting overnight. No premedication was given. All patients received four ECT sittings consecutively and the anaesthetic agents were alternated. The patients were randomly allocated to receive either 2.5% Thiopentone (T) or Propofol 1% (P) on the 1st ECT. Patients were preoxygenated for three minutes with 100% oxygen. After administering Glycopyrrolate 0.2 mg Thiopentone (3mg/kg) or Propofol (1.5mg/kg) was administered through an indwelling cannula in a vein on the dorsum of the hand. Suxamethonium 0.5mg/kg was given, the patients lungs were inflated with 100% oxygen through a face mask and bag. When fasiculations subsided a mouth prop was inserted and a bitemporal ECT was performed (cerebral simulator ME-1, 26677 TE). The current volts was kept constant at 110 Volts throughout the study. The mouth prop was changed to Guedel’s airway after the seizure and ventilation assisted with face mask with 100% oxygen until return of spontaneous ventilation. Patients were monitored in the recovery room for half an hour and shifted to the ward. All monitoring was carried out by the same doctor who was blinded to the anaesthetic agent used. All patients have continuous ECG monitoring and noninvasive BP monitoring (ARTEMA MM 214) by an automatic BP machine. Oxygen saturation and heart rate were also monitored. Seizure duration was observed by isolating one limb with a blood pressure cuff raised to 20mm Hg above the systolic BP before administration of the muscle relaxant. Seizure duration was noted as the time from ECT to the end of seizure. The recovery time was noted as the time from injecting the medication to opening of eyes on command. The heart rate and BP was monitored at preinduction and at 1 min, 3 min and 5 min after conclusion of ECT. The data was analysed using the students paired t test.
RESULTS Heart Rate: There was a maximal increase in the heart rate in group T patients in the third minute (20.04%) (111.01±17.62). Group P patients also showed a maximal increase in the heart rate in the third minute (10.82%)(99.41±16.97). Group T patients had much higher increase than Group P patients. The difference is significant (p value 0.000) (Graph 1, 2). Systolic Blood Pressure: There was a maximal increase in systolic blood pressure in Group T (33.06%) (165.79 ±23.87) and Group P (17.36%) (139.57 ± 16.28) in the third minute. The increase in blood pressure in Group T was more than Group P. This difference was statistically significant (p value 0.000) (Graph 3, 4) Diastolic Blood Pressure: There was a maximal increase in group T and Group P in the first minute (33.95 %) (102.42 ±20.24) and Group P (17.36%) (88.18 ±15.52) in the first minute. This increase in blood pressure was higher in Group T. The difference was statistically significant (p value 0.000). (Graph 5, 6) Seizure Duration: Group T patients had a seizure duration of 27.98 ± 10.97 seconds, when compared to Group P patients 19.65± 8.46 seconds. The difference was statistically significant (p value 0.00) (Graph 7). Recovery Time: Group T patients had a prolonged recovery (10.39min±5.74) than Group P patients who had a faster recovery (7min±1.87). This was statistically significant (p value 0.000) (Graph 8).
DISCUSSION From 1963, ECT was modified by the use of intravenous anaesthetic agents, there has been a need to find the ideal agent to attenuate the effects of ECT on the brain and the cardiovascular system. Many studies have been conducted comparing various medications like Thiopentone, Methohexitone, Etomidate and Propofol during ECT. In our study an attempt has been made to compare the recovery profile, haemodynamic response and the seizure durations following the use of thiopentone and propofol. Breakdown of the blood brain barrier has been shown to occur in rats during epileptic seizures because of acute hypertension rather than the seizure per second. There is also good correlation between the maximal increase of systolic BP after electroconvulsive therapy and cognitive defect. Severe elevations in BP and heart rate would also increase the risk of myocardial infarction or stroke in susceptible patients. BP and heart rate increase is significantly higher with Thiopentone. It is therefore essential to lessen the Haemodynamic response during ECT. In our study Propofol has proved to be a safe anaesthetic agent with milder haemodynamic changes as similar to trials conducted by Zaidi et al6 and Kirby et al7. The effect of Propofol on seizure activity is not clear. Recent reports have suggested a possible relationship of Propofol to seizure and opisthotonus. Avramov et al8 and Rouse et al9 compared Propofol and Methohexitone for ECT and have shown a shorter duration of seizure with Propofol. We found a similar effect in this study with Propofol compared to Thiopentone. Geretsegger et al10 showed the difference in seizure duration is unrelated in seizure quality measures. This study was further supported by Fear C.F et al11. They concluded that reduced seizure duration may not be relevant and it is not necessarily contraindicated as an induction agent for ECT. Although seizure duration was less with Propofol as Mitchell et al12 aptly stated, it is premature to abandon the use of Propofol as an anaesthetic agent in ECT due to this disadvantage. It might be particularly indicated when hypertension during ECT may be detrimental to the patient since this complication is attenuated by the drug. In conclusion it is proved that Propofol has better haemodynamic response, heart rate, systolic and diastolic blood pressure along with early recovery than Thiopentone. Although Propofol has a shorter seizure duration, its advantages outweigh the disadvantages. Thus proving that Propofol is an ideal anaesthetic agent for ECT.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.