 Home
Home
|
Table of Content - Volume 1 Issue 2 - February 2016
Role of Vitamin - D in cases of COPD
Shiv Kumar1*, Amitabh Batsh2, Gorachand Bhattacharya3
{1Associate Professor, Department of TB and Chest} {2IIIrd Yr. PGT, 3Professor, Department of Biochemistry} MGM, Medical College and LSK Hospital, Kishanganj-855107, Bihar, INDIA. Email: kajal6160@gmail.com
Abstract Problem statement: Chronic obstructive pulmonary disease (COPD) is one of the most common lung diseases. There are two main forms of COPD: Chronic bronchitis is identified by a long-term cough with mucus and Emphysema is a slow destruction of the lungs over time. Most people with COPD have a combination of both conditions. Symptoms include cough with mucus, shortness of breath that worsens with mild activity, fatigue, frequent respiratory infections, and wheezing. Symptoms vary and become worse at times. Methods: Patient were attending Chest and TB OPD of the MGM Medical College and L S K Hospital Kishanganj Bihar diagnosed to be suffering from COPD by X-Ray, PFT and clinical findings will be selected for the study. Total no of cases ~50 were taken for study. Healthy individuals not suffering from any infection or serious disease were selected as control group. Results: Study was to access the Vitamin-D status in COPD subjects because recent evidence suggests Vitamin-D has potent exo-skeletal effects. Such as suppression of inflammation and strengthening of mucosal immunity by synthesis of anti-microbial peptides. We designed our study to carry out a case control study in COPD subjects after clinical and radiological diagnosis from the Chest and TB Department. Routine biochemical parameters were also investigated. Routine blood glucose level among the test and control group were not statistically significant p Value (0.506). Blood urea and serum creatinine level as observed in our study were not statistically significant, p Value <0.01 for both the parameters. We observed a significantly low value of 25-Hydroxy Vitamin-D in subjects of COPD and the level was in deficient range for control group. We found optimum level of 25-Hydroxy Vitamin-D with significant p Value <0.001. Conclusion: Available data from observational studies indicate that reduced level of 25Hydroxy vitamin-D is associated with increased risk of respiratory tract infection. Some results were from different randomised control trials on the protective role of vitamin-D against respiratory tract infection are inconclusive, so more studies are required. Key Words: COPD, 25Hydroxy vitamin-D.
INTRODUCTION According to various studies, there is a strong relationship between vitamin D levels and forced air capacity. This includes the total amount of air forced from the lungs after taking the deepest breath possible. It also includes the amount of air forced during the first second of exhalation. Vitamin D deficiency occurs frequently in COPD. This is shown in a few studies: In Indian people hospitalized for an acute attack of COPD had higher death rates between December and January. Rates of viral respiratory infections are highest at that time because there is less sunlight.1 Ultraviolet-B (UVB) light and vitamin D may reduce the risk of COPD flare-ups. Two studies reported that farmers had lower rates of COPD attacks. However, farmers in general have higher rates of COPD, possibly because they are exposed to more organic matter and chemicals.2 Vitamin D may protect against COPD flare-ups by- Protecting the body against viral and bacterial infections. These infections often trigger COPD attacks and Reducing compounds in the body that destroy tissues. This includes matrix metalloprotease-9 (MMP-9). MM-9 may contribute to COPD.3 Those with COPD have an increased risk of osteoporosis. Vitamin D can reduce the risk of osteoporosis. People with COPD should supplement with vitamin D and calcium. Doses of 800 international units (IU) (20 mcg)/day of vitamin D plus calcium have been shown to provide some protection against osteoporosis.4 Based on the evidence, vitamin D levels above 30–40 ng/mL (75-–100 nmol/L) may reduce the risk of COPD. To reach these levels, most people need to take 1000–5000 international units (IU) (25–125 mcg)/day of vitamin D3. This is the active form of vitamin D produced under the skin. However, there is considerable variation from person to person.5 To determine proper dosage, vitamin D blood levels should be measured before and several months after taking vitamin D3 supplements or increasing UVB exposure.Recent years have seen a growing interest in extra-osseous actions of vitamin D. The physiology of vitamin D, the pathophysiological aspects associated with its deficit and the evidence of its pathogenic role in respiratory diseases. Investigators of the study hoped that high doses of vitamin D would reduce the number of exacerbations in these patients that often result in hospital stays. However, they found only a limited benefit from vitamin D supplements. Despite blood levels of vitamin D rising significantly in those taking the supplement, researchers found no significant difference in the time before an exacerbation or the number of flare-ups between these patients and those receiving the placebo. The term vitamin D is, unfortunately, an imprecise term referring to one or more members of a group of steroid molecules. Vitamin D3, also known as cholecalciferol is generated in the skin of animals when light energy is absorbed by a precursor molecule 7-dehydrocholesterol. Vitamin D is thus not a true vitamin, because individuals with adequate exposure to sunlight do not require dietary supplementation. There are also dietary sources of vitamin D, including egg yolk, fish oil and a number of plants. The plant form of vitamin D is called vitamin D2 or ergosterol. However, natural diets typically do not contain adequate quantities of vitamin D, and exposure to sunlight or consumption of foodstuffs purposefully supplemented with vitamin D are necessary to prevent deficiencies.
MATERIAL AND METHODS Type of Study: Case and control study. Study Area: Department of Biochemistry MGM Medical College and L S K Hospital, Kishanganj, Bihar in collaboration with Department of Medicine (TB and Chest) of same institution. Study Duration: The duration of study was from Jan 2015 to Feb 2016. Study population and sampling frame: A synopsis of this research study design consists of Introduction, Aims and Objective sand protocol were submitted for approval after getting the permission from the Ethical Committee, M.G.M. Medical College and L.S.K. Hospital, Kishanganj, Bihar. Eligibility of the study population: Patient were attending Medical OPD of the MGM Medical College and L S K Hospital Kishanganj Bihar diagnosed to be suffering from COPD by X-Ray, PFT and clinical findings will be selected for the study. Total no of cases ~50 were taken for study. Healthy individuals not suffering from any infection or serious disease were selected as control group. Investigation
Inclusion Criteria: There are reports from different corners of globe that vitamin D is associated with chronic diseases that includes COPD. A low serum level of vitamin has been reported but these reports are inconclusive. Exclusion Criteria: Diabetes Mellitus, Hypertension, Tuberculosis patients were excluded in our study.
RESULTS
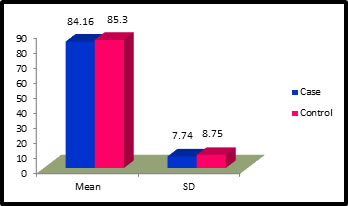
Table 1: Distribution of Glucose among case and control
Figure 1: Distribution of Glucose among case and control
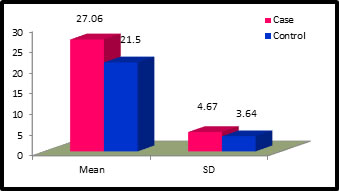
Table 2: Distribution of Urea among case and control
Figure 2: Distribution of Urea among case and control
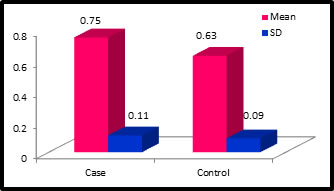
Table 3: Distribution of Creatinine among case and control
Figure 3: Distribution of Creatinine among case and control
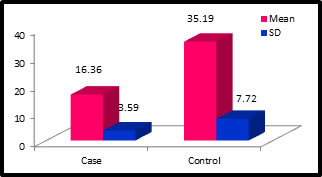
Table 4: Distribution of Vitamin-D among case and control
Figure 4: Distribution of Vitamin-D among case and control
DISCUSSION The object of our study was to access the Vitamin-D status in COPD subjects because recent evidence suggests Vitamin-D has potent exo-skeletal effects. Such as suppression of inflammation and strengthening of mucosal immunity by synthesis of anti-microbial peptides. Available data from observational studies indicate that reduced level of 25Hydroxy vitamin-D is associated with increased risk of respiratory tract infection. Some results were from different randomised control trials on the protective role of vitamin-D against respiratory tract infection are inconclusive, so more studies are required. We designed our study to carry out a case control study in COPD subjects after clinical and radiological diagnosis from the Medicine Department. Routine biochemical parameters were also investigated, routine blood glucose level among the test and control group were not statistically significant p Value (0.506). Blood urea and serum creatinine level as observed in our study were not statistically significant, p Value <0.01 for both the parameters. We observed a significantly low value of 25-Hydroxy Vitamin-D in subjects of COPD and the level was in deficient range for control group. We found optimum level of 25-Hydroxy Vitamin-D with significant p Value <0.001. Peter Bergman et. al. (2012)6 reported that supplementation with Vitamin D3 may reduce disease burden in patients with respiratory tract infection. They conducted randomised control trial with supplementation of vitamin D3 and concluded that vitamin D3 supplementation may prevent respiratory tract infection and reduce antibiotic consumption, particularly in patients with hypogammaglobinaemia or with increased frequency of respiratory tract infection.
CONCLUSION Our study included 50 COPD patients and 50 healthy controls. 25 Hydroxy vitamin D levels in COPD cases were in deficient range as compared to control group having an optimal range of 25 Hydroxy vitamin D. This observation has been similar to work done by other researchers. We conclude with the idea that COPD may be manifested by a low 25 Hydroxy vitamin D level and calcitrol may be supplemented in subjects of COPD. Limitation of our study is small sample size and patients are chosen from a selected part of area. Vit-D could be beneficial for the prevention or therapy of important lung diseases. So in future this study would be carried with a larger sample size, within variety of population and with wider parameters.
REFERANCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.