 Home
Home
|
Table of Content - Volume 1 Issue 3 - March 2016
Incidence and profile of patients suffering from pneumonia observed in tertiary care institute
Khemchandra Dhanraj Borole1*, Dinesh Eknath Nehete2
1,2Associate Professor, Department of Medicine, Dr Ulhas Patil Medical College, Jalgaon, Maharashtra, INDIA. Email: drkhem.b@gmail.com
Abstract Background: Pneumonia is an inflammatory condition of the lung affecting primarily the microscopic air sacs known as alveoli. It is usually caused by infection with viruses or bacteria and less commonly other microorganisms, certain drugs and other conditions such as autoimmune diseases. Aims and Objective: To study the incidence, profile and seasonal trend of pneumonia observed among the patients admitted in tertiary care center. Materials and Method: All the cases admitted in the institute during March 2014 to Feb. 2015 were selected. Out of them cases of pneumonia were studied in detail. During the study duration total 6791 patients were admitted in the institute, out of them 243 were suffering from pneumonia. The detail information of each case was obtained from the record and entered in a prestructured proforma, which included age, sex and presenting complaints. Details about general and systemic examination were also recorded. Data records obtained also included variables as month of admission, month of discharge and year of admission. Results: Out of 6791 admission 243 were diagnosed to be suffering from pneumonia. Thus the incidence of pneumonia was 35.78/1000patients. The most common presenting feature was fever, cough, tachycardia and chest pain (95.88%, 97.94%, 88.89% and 69.14% respectively). Majority of the patients suffering from pneumonia were young adults in the age group of 21 to 40 years (53.5%) followed by 41 to 60 years (32.51%) and ≥61years (12.76%). The incidence of pneumonia among male was more as compared to female. While studying the seasonal trend of pneumonia, it was seen that the incidence of pneumonia was more in winter as compared to summer season. Conclusion: The incidence of pneumonia was 35.78/1000patients. The incidence was more in elderly male with peak incidence in winter season. Key Words: pneumonia, incidence, seasonal variation, clinical profile.
INTRODUCTION Pneumonia is an inflammatory condition of the lung affecting primarily the microscopic air sacs known as alveoli.1,2 It is usually caused by infection with viruses or bacteria and less commonly other microorganisms, certain drugs and other conditions such as autoimmune diseases.1,3 According to World Health Organization (WHO) global burden of disease study it has been estimated that lower respiratory tract infections (LRTIs), which include CAP, 429.2 million episodes of illness worldwide and accounts for 94.5 million disability adjusted life years (DA LYs). In adults aged over 59 years, it causes 1.6 million deaths annually.4 According to a population-based epidemiological study conducted in Europe has shown that CAP has the highest incidence in winter and spring.5 The disease occurs more in males with ratio of 1.4: 1. This pattern is also maintained in hospital data (1.85: 1)6. In almost all papers, the incidence is shown to be increased with age. In an epidemiological survey of individuals age 15–64 years, an incremental annual incidence rate was observed (1.12–3.16 per 1000 inhabitants). Patients suffering from community acquired pneumonia and requiring hospital treatment are usually elderly persons and persons with underlying chronic obstructive pulmonary disease (COPD), such as chronic bronchitis (not emphysema); and individuals with severe CAP related to underlying cardiopulmonary function, immune status, or pathogen virulence.7 Typical presentation of pneumonia include cough, chest pain, fever, and difficulty breathing8 and Diagnostic tools include x-rays and culture of the sputum.
MATERIALS AND METHOD The present retrospective study was conducted in the department of medicine of Dr Ulhas Patil Medical College, Jalgaon. For the purpose of study all the cases admitted in the institute during March 2014 to Feb. 2015 were selected. Out of them cases of pneumonia were studied in detail. During the study duration total 6791 patients were admitted in the institute, out of them 243 were suffering from pneumonia. The detail information of each case was obtained from the record and entered in a prestructured proforma, which included age, sex and presenting complaints. Details about general and systemic examination were also recorded. Data records obtained also included variables as month of admission, month of discharge and year of admission. The collected data was entered in Microsoft excel and was analyzed and presented with appropriate tables and graphs.
RESULTS Table 1: Incidence of pneumonia
There were total 6791 admissions in medicine inpatients department in the study duration. It was observed that out of 6791 admission 243 were diagnosed to be suffering from pneumonia. Thus the incidence of pneumonia was 35.78/1000patients.
Table 2: Distribution of patients according to clinical features
* Multiple responses observed It was evident from the table that the most common presenting feature was fever, cough, tachycardia and chest pain (95.88%, 97.94%, 88.89% and 69.14% respectively).
Table 3: Distribution of cases according age and sex
It was seen that majority of the patients suffering from pneumonia were young adults in the age group of 21 to 40 years (53.5%) followed by 41 to 60 years (32.51%) and ≥61years (12.76%). The incidence of pneumonia among male was more as compared to female. The age wise distribution of cases among the both sex was nearly same.
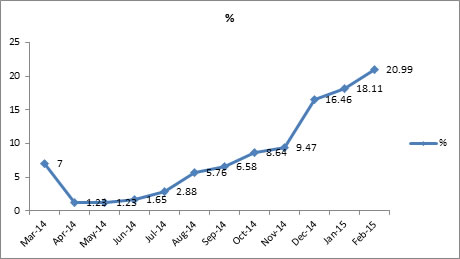
Table 4: Monthwise distribution of cases
While studying the seasonal trend of pneumonia, it was seen that the incidence of pneumonia was more in winter as compared to summer season.
DISCUSSION The present retrospective study was conducted in the department of medicine of Dr Ulhas Patil Medical College, Jalgaon with objective to study the incidence and clinical profile of patients suffering from pneumonia. There were total 6791 admissions in medicine inpatients department in the study duration. It was observed that out of 6791 admission 243 were diagnosed to be suffering from pneumonia. Thus the incidence of pneumonia was 35.78/1000patients. In a study by Angel Vila-Corcoles9 the incidence rate of CAP observed in population was 14 cases per 1000 elderly person-years. As compared to present study J. Almirall et al10 observed much less incidence (1.62 cases per 1000 inhabitants) in their study. In England incidence of community-acquired pneumonia has been reported, as 5 per 1,000 persons11, whereas in Finland as 9 per1000 inhabitants >14 yrs of age13. In a study from Spain by Santos De Unamuno et al14 reported an incidence rate of 1.8 per 1,000 inhabitants >14 yrs of age. In another study by Almirall J et al reported an incidence rate of 2.6 per 1,000 persons >13 yrs of age was found14. It was evident from the table that the most common presenting feature was fever, cough, tachycardia and chest pain (95.88%, 97.94%, 88.89% and 69.14% respectively). Similar findings were also observed by Bashir Ahmed Shah et al15 in their study. They observed that the maximum number of patients presented with fever (95%), cough (99%), tachycardia (92%), pleuritic chest pain (75%) and sputum production(65%), and leucocytosis (43%). Angel Vila-Corcoles9 studied the cases of pneumonia and observed that cough was present in 68.1% cases, fever in 69.8%, dyspnoea in 53.9%, expectoration in 58.1%, pleural pain in 47.4% and crepitations in 83.5%. It was seen that majority of the patients suffering from pneumonia were young adults in the age group of 21 to 40 years (53.5%) followed by 41 to 60 years (32.51%) and ≥61years (12.76%). Thus we could state that the incidence of community-acquired pneumonia was higher in elderly. This period of life is characterized by the occurrence of chronic and debilitating conditions, which tend to be more frequent in males and have been found to be a major risk factor for community-acquired pneumonia16. The incidence of pneumonia among male was more as compared to female. Similar finding were also reported by J. Almirall et al10 and Bashir Ahmed Shah et al15. It was also seen that the age wise distribution of cases among the both sex was nearly same. While studying the seasonal trend of pneumonia, it was seen that the incidence of pneumonia was more in winter as compared to summer season. In a study Fransen H et al17 reported peak number of hospitalizations due to pneumonia was observed in the spring and winter seasons. FOY et al18 studied the occurrence of pneumonia over a successive 5 year period and observed peaks occurred in the spring and in the winter. Mohammad Zeeshan Raza19 also observed peak incidence in spring and winter.
CONCLUSION The incidence of pneumonia was 35.78/1000patients. The incidence was more in elderly male with peak incidence in winter season.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.