 Home
Home
|
Table of Content - Volume 1 Issue 3 - March 2016
Outcome of pneumonia among the patients: A retrospective hospital based study
Chandrayya Achanna Kante1*, Khemchandra Dhanraj Borole2
1Assistant Professor, 2Associate Professor, Department of Medicine, Dr Ulhas Patil Medical College, Jalgaon, Maharashtra, INDIA. Email: drcakante@gmail.com
Abstract Background: Pneumonia is an infection caused primarily by bacteria or viruses and less commonly by fungi and parasites. More than 100 strains of infectious agents have been identified but only a few of them are responsible for the majority of the cases. Aims and Objectives: To study the outcome of community acquired pneumonia admitted in the tertiary care institute. Materials and Method: In the present retrospective study all the cases of pneumonia admitted in the institute during March 2014 to Feb. 2015 were selected. Patients were included in the data analysis if they had a primary admission diagnosis of pneumonia irrespective of the gender, race, or residence. Thus total 243 cases were enrolled in the present study. The detail information of each case was obtained from the record and entered in a prestructured proforma, which included age, sex and presenting complaints. Details about general and systemic examination were also recorded. Data records obtained also included variables as month of admission, month of discharge and year of admission. Details about the treatment given, total days of hospital stay and outcome of the disease were also recorded. Results: Majority of the patients suffering from pneumonia were young adults in the age group of 21 to 40 years (53.5%) followed by 41 to 60 years (32.51%) and ≥61years (12.76%). The incidence of pneumonia among male was more as compared to female. The most common presenting feature was fever, cough, tachycardia and chest pain (95.88%, 97.94%, 88.89% and 69.14% respectively). The mean duration of hospital stay was 9.25±2.15days. In the present study the majority of the patients (90.12%) were recovered after the effective management. 5.76% patients improved and were discharged and advised for regular follow up. The mortality rate due pneumonia was observed to be 0.82%. Conclusion: Thus we conclude that the mortality rate due pneumonia was observed to be 0.82%. The mean duration of hospital stay was 9.25±2.15days. Key Words: pneumonia, outcome, morality rate, hospital stay.
INTRODUCTION Pneumonia is an infection caused primarily by bacteria or viruses and less commonly by fungi and parasites. More than 100 strains of infectious agents have been identified but only a few of them are responsible for the majority of the cases. Mixed infections with both viruses and bacteria have been observed more commonly in children (up to 45%) as compared to adults (15%)1 and causative agent may not be isolated in approximately half of cases despite careful testing.2 In recent years, both the epidemiology and treatment of pneumonia have undergone changes. Pneumonia is increasingly common among older patients and those with co-morbidity like COPD, DM, renal failure, congestive heart failure, CLD and other conditions.3 Community-acquired pneumonia (CAP) remains a common and serious illness despite the availability of potent new anti-microbials and effective vaccines. In the United States, pneumonia is the sixth leading cause of death from infectious diseases.4,5 Most of the types of bacterial pneumonia will stabilize in 3–6 days with treatment. whereas it often takes a few weeks before most symptoms resolve.6 X-ray finding typically clear within four weeks. The duration of recovery is more in the elderly or in people with other lung problems. In persons requiring hospitalization, mortality may be as high as 10%, and in those requiring intensive care it may reach 30–50%.7 Pneumonia is the most common hospital-acquired infection that causes death. In the present retrospective record based study we tried to study the outcome of pneumonia admitted in the present study institute during one year.
MATERIALS AND METHOD The present retrospective study was conducted in the department of medicine of Dr Ulhas Patil Medical College, Jalgaon. For the purpose of study all the cases admitted in the institute during March 2014 to Feb. 2015 were selected. Patients were included in the data analysis if they had a primary admission diagnosis of pneumonia irrespective of the gender, race, or residence. Thus total 243 cases were enrolled in the present study. The detail information of each case was obtained from the record and entered in a prestructured proforma, which included age, sex and presenting complaints. Details about general and systemic examination were also recorded. Data records obtained also included variables as month of admission, month of discharge and year of admission. Details about the treatment given, total days of hospital stay and outcome of the disease were also recorded. The collected data was entered in Microsoft excel and was analyzed and presented with appropriate tables and graphs.
RESULTS Table 1: Distribution of cases according age and sex
Table 2: Distribution of patients according to clinical features
*Multiple responses observed It was evident from the table that the most common presenting feture was fever, cough, tachycardia and chest pain (95.88%, 97.94%, 88.89% and 69.14% respectively).
Table 3: Distribution of patients according to Hospital stay
It was seen that majority of the patients (70.78%) required 6 to 10 days of hospital stay followed by 11-15 days (23.87%). The mean duration of hospital stay was 9.25±2.15days.
Table 4: Distribution of patients according to Outcome
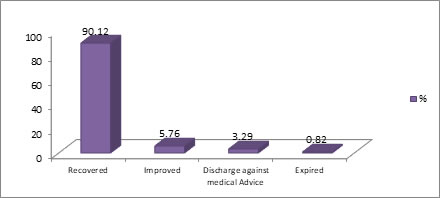
Figure 1: Distribution of patients according to Outcome
In the present study the majority of the patients (90.12%) were recovered after the effective management. 5.76% patients improved and were discharged and advised for regular follow up. The mortality rate due pneumonia was observed to be 0.82%.
DISCUSSION The objective of the present study was to study the outcome of pneumonia among the patients admitted in the tertiary care institute. For this purpose we conducted a retrospective record based study in the department of medicine of Dr Ulhas Patil Medical College, Jalgaon. It was seen that majority of the patients suffering from pneumonia were young adults in the age group of 21 to 40 years (53.5%) followed by 41 to 60 years (32.51%) and ≥61years (12.76%). Thus we could state that the incidence of community-acquired pneumonia was higher in elderly. This period of life is characterized by the occurrence of chronic and debilitating conditions, which tend to be more frequent in males and have been found to be a major risk factor for community-acquired pneumonia8. The incidence of pneumonia among male was more as compared to female. Similar finding were also reported by J. Almirall et al9 and Bashir Ahmed Shah et al10. It was evident from the table that the most common presenting feature was fever, cough, tachycardia and chest pain (95.88%, 97.94%, 88.89% and 69.14% respectively). Similar findings were also observed by Bashir Ahmed Shah et al10 in their study. They observed that the maximum number of patients presented with fever (95%), cough (99%), tachycardia (92%), pleuritic chest pain (75%) and sputum production (65%), and leucocytosis (43%). Angel Vila-Corcoles11 studied the cases of pneumonia and observed that cough was present in 68.1% cases, fever in 69.8%, dyspnoea in 53.9%, expectoration in 58.1%, pleural pain in 47.4% and crepitations in 83.5%. It was seen that majority of the patients (70.78%) required 6 to 10 days of hospital stay followed by 11-15 days (23.87%). The mean duration of hospital stay was 9.25±2.15days. J. Almirall et al9 reported a mean hospital stay of 11.7±10.1 days in their study. In the present study the majority of the patients (90.12%) were recovered after the effective management. 5.76% patients improved and were discharged and advised for regular follow up. The mortality rate due pneumonia was observed to be 0.82%. As compared to the present study J. Almirall et al9 observed higher mortality rate (5%). In population surveys carried out in the USA, the mortality rate reached 24.1 per 100,000 inhabitants, in fifth place after cardiovascular, neoplastic, cerebrovascular, and chronic bronchitis for largest mortality rate12. Bashir Ahmed Shah et al10 reported the mortality rate of 14% in their study. The mortality rate of CAP in various hospital based studies is variable, being 5.7% in a British Thoracic Society multi-centric study13 to a higher mortality of (21-25%) in other studies.14,15
CONCLUSION Thus we conclude that the mortality rate due pneumonia was observed to be 0.82%. thw mwan duration of hospital stay was 9.25±2.15days.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.