 Home
Home
|
Table of Content - Volume 3 Issue 1 - July 2016
Study of symptomatology in patients with chronic obstructive lung diseases at a tertiary care hospital
Gaurav R Dubey1, Anjali S Deshmukh2*, Vijay R Kapse3
1Assistant Professor, Department of TB and Respiratory Medicine, Dr PDMMC Amravati, Maharashtra, INDIA. 2Assistant Professor, 3Associate Professor, Department of Medicine, Dr.S.C.G.M.C.Nanded, Maharashtra, INDIA. Email: dr.dranju@rediffmail.com
Abstract Background: Chronic Obstructive Pulmonary Disease (COPD) is manifested by chronic cough, sputum production, wheezing and, in later stages, dyspnea, poor exercise tolerance, and signs/symptoms of right-sided heart failure. Symptomatic COPD affects more than 5 percent of the adult population, is the fourth leading cause of death, and the twelfth leading cause of morbidity in the United States. Amis and Objective: To study the symptomatology in patients with chronic obstructive lung diseases at a tertiary care hospital Material and Method: All the patients of chronic obstructive lung diseases attending the respiratory OPD during the January 2016 to June 2016 were enrolled in the present study. The patients not willing to participate the study were excluded. The detail demographic characteristics such as age, sex, occupation etc were inquired and were entered a prestructured proforma. The associated risk factors were also investigated and were recorded. The presenting symptoms were also recorded. The collected data was entered in Microsoft excel and was analyzed and presented with appropriate tables and graphs. Results: The mean age of the study patients was 46.26±16.71 years. Majority of the patients were male (59.32%). 25.99% patients in the present study were labourer whereas farmers were 19.77%. Majority of the women were house wives. 28.81% patients were having smoking habit. Majority of them were using bidi and 5 were female. Out of total 72 female in the present study 33 were exposed to chullah smoke. Breathlessness (92.66%) followed by cough (79.66%) were the most common presenting complaint. It was seen that the in majority of the patients the symptoms were less one month duration (46.89%). Conclusion: Thus we conclude that COPD was observed common among the male population more than 40 years of age. Smoking and Exposure to chullah smoke and occupation such as labourer, farmers and house wives who are exposed dust are at risk of developing COPD. The most common presenting symptom among the study patients was breathlessness followed by cough, chest tightness and wheezing. Key Words: Chronic obstructive lung diseases, symptoms, risk factors.
INTRODUCTION According to global initiative for chronic obstructive lung disease, chronic obstructive pulmonary disease (COPD) is defined as preventable and treatable disease with some significant extra-pulmonary effects,1 which may contribute to the severity in individual patients. COPD represents a significant and increasing healthcare concern as a leading cause of morbidity and mortality, worldwide. COPD is responsible for approximately 2.75 million deaths worldwide.2 Moreover, COPD at present is 12th leading cause of disability worldwide, and is expected to be the fifth leading cause of disability by 2020.3,4 Chronic Obstructive Pulmonary Disease (COPD) is manifested by chronic cough, sputum production, wheezing and, in later stages, dyspnea, poor exercise tolerance, and signs/symptoms of right-sided heart failure. Symptomatic COPD affects more than 5 percent of the adult population, is the fourth leading cause of death, and the twelfth leading cause of morbidity in the United States.5,6 Over the last couple of decades, there has been a fair deed of published data on the extra pulmonary manifestations of COPD.7,8 The consensus statement of GOLD has also defined COPD as a disease with significant extra pulmonary manifestations. Estimates of the population attributable fraction of tobacco smoking as a cause of COPD vary by age and population setting10, although more recent estimates in those aged 30-69 years, 54% for men and 24% for women, are probably accurate and less than the widely quoted 80-90% in the 1984 US Surgeon General Report11. Attributable fractions are higher in industrialized countries than developing countries10, and other risk factors are also important, including exposure to biomass smoke, occupational exposures to dust and fumes, history of pulmonary tuberculosis, outdoor air pollution, and poor socioeconomic status12 or chronic asthma13. However smoking remains the most important cause of COPD in western countries. Around 50% of smokers eventually develop COPD, although the risk falls by about half following smoking cessation11.
MATERIAL AND METHOD The present study was conducted in the department of respiratory medicine of Statperson medical college. All the patients of chronic obstructive lung diseases attending the respiratory OPD during the January 2016 to June 2016 were enrolled in the present study. The patients not willing to participate the study were excluded. The detail demographic characteristics such as age, sex, occupation etc were inquired and were entered a prestructured proforma. The associated risk factors were also investigated and were recorded. The presenting symptoms were also recorded. The collected data was entered in Microsoft excel and was analyzed and presented with appropriate tables and graphs.
RESULTS Table 1: Age, sex and occupation distribution of study patients
In the present study total 177 patients of chronic obstructive pulmonary disease were studied. It was seen that the patients were in the range of 14 – 81 years and majority of the patients were in the age group of 31-40 years of age followed by 51-60 years and 61-70 years. The mean age of the study patients was 46.26±16.71 years. It was seen that majority of the patients were male (59.32%) with male: female ratio of 1.46:1. It was observed that 25.99% patients in the present study were labourer whereas farmers were 19.77%. Majority of the women were house wives.
Table 2: Distribution of study patients according associated to risk factors
It was seen that 51 (28.81%) patients were having smoking habit. Majority of them were using bidi. And 5 were female. It was seen that out of total 72 female in the present study 33 were exposed to chullah smoke. Past history of tuberculosis was reported by 18.08% patients. Family history of atopy was reported by 13.56% patients.
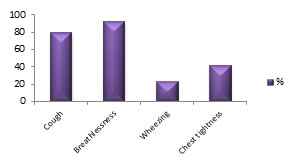
Table 3: Distribution of patients according presenting symptoms
The most common presenting complaint among the study patients was breathlessness (92.66%) followed by cough (79.66%), chest tightness (23.16%) and wheezing (23.16%). Figure 1: Distribution of patients according presenting symptoms Table 4: Distribution of patients according duration symptoms
It was seen that the in majority of the patients the symptoms were less one month duration (46.89%).
DISCUSSION The present study was conducted in the department of respiratory medicine of ABC medical college with the aim to Study of symptomatology in patients with chronic obstructive lung diseases. In the present study total 177 patients of obstructive lung disease were enrolled and were studied in detail. It was seen that the patients were in the range of 14 – 81 years and majority of the patients were in the age group of 31-40 years of age followed by 51-60 years and 61-70 years. The mean age of the study patients was 46.26±16.71 years. COPD prevalence is higher in subjects older than 40 years of age compared with those younger than 40 years, regardless of the diagnostic criteria used14. It was seen that majority of the patients were male (59.32%) with male: female ratio of 1.46:1. The role of sex in determining COPD risk remains unclear14. In the past, most studies showed that COPD prevalence and mortality were greater among men than women. More recent studies showed that the sex difference in COPD prevalence tends to disappear15,16. Regarding COPD incidence, most17-19 but not all20 studies found a higher risk in men than in women. It was observed that 25.99% patients in the present study were labourer whereas farmers were 19.77%. Majority of the women were house wives. Exposure to occupational dusts and chemicals and air pollution are important risk factors and can cause COPD independently of tobacco smoke21. Such exposure results in inflammation, a key factor in the pathogenesis of COPD. Chronic inflammation throughout the airways, parenchyma, and pulmonary vasculature are hallmarks of the disease process and lead to the pathologic changes characteristic of COPD. It was seen that 51 (28.81%) patients were having smoking habit. Majority of them were using bidi. And 5 were female. Association of cigarette smoking with COPD is well established.ref2-15 According to the American Lung Association, risk of death from disease is 13 times more higher in smokers as compared to non-smokers.22,23 Previous studies have found that cigarette smoking is an important risk factor for COPD mortality and that smoking cessation reduces the risk of COPD mortality24-29. Past history of tuberculosis was reported by 18.08% patients. Family history of atopy was reported by 13.56% patients. It was seen that out of total 72 female in the present study 33 were exposed to chullah smoke. According to a systematic review and meta-analysis done in 2010, positive associations were found between the exposure to smoke of solid fuels and COPD and chronic bronchitis. Among different types of smoke ejecting fuels, exposure to wood smoke, while performing domestic work, imposes a greater risk of development of COPD and chronic bronchitis than other fuels.1 The most common presenting complaint among the study patients was breathlessness (92.66%) followed by cough (79.66%), chest tightness (23.16%) and wheezing (23.16%). The findings were comparable with the findings in the study by Jain NK et al.30 In a study by Kamdar DJ et al31 88% patients had cough, while 68% had cough with sputum production at the time of presentation.
CONCLUSION Thus we conclude that COPD was observed common among the male population more than 40 years of age. Smoking and Exposure to chullah smoke and occupation such as labourer, farmers and house wives who are exposed dust are at risk of developing COPD. The most common presenting symptom among the study patients was breathlessness followed by cough, chest tightness and wheezing.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.