 Home
Home
|
Table of Content - Volume 3 Issue 3- September 2016
A study of clinical features and outcome of patients with acute renal failure requiring dialysis at department of medicine of tertiary health care centre
Vinod Ramchandra Baviskar1, Janrao Bhaurao Rajput2*
1,2Associate Professor, Department of General Medicine, Dr. Ulhas Patil Medical College and Hospital, Jalgaon, Maharashtra, INDIA. Email: drrajputjb@gmail.com
Abstract Background: Acute renal failure (ARF), now increasingly referred to as “acute kidney injury” (AKI), is characterized by sudden (i.e., hours to days) impairment of kidney function. Acute kidney injury (AKI) is defined as a rapid (over hours to weeks) and usually reversible decline in glomerular filtration rate (GFR) that can occur either in the setting of previously normal renal function (“classical” AKI) or in a patient with pre-existing chronic kidney disease (acute-onchronic renal failure; ACRF). Aims and Objectives: To Study the Clinical features and Outcome of patients suffering from Acute Renal Failure requiring dialysis reporting to the Department of medicine of Tertiary care centre. Materials and Methods: In the present hospital based retrospective cross-sectional study all the adult AKI patients who required haemodialysis and admitted during the January 2016 to December 2016 were enrolled in the study. The medical records of all patients admitted during the study period were studied. All patients of age 14 and above with AKI and have been dialyzed at least once during the study period were included. In the hospital patients of age 14 and above are considered as “adults” and admitted to the adult patient wards. Those patients who had dialysis for overdose of dialyzable drugs; those who were under the age of 14 or had incomplete or missing records were excluded. Data on sociodemographic details, clinical features and causes associated with AKI were recorded on a prestructured proforma. Results: Majority of the patients requiring dialysis with acute kidney disease were young with age less than 40 years of age. Male patients were 59.57%. 70.21% patients were from urban area. Oligouria (80.85%), edema (65.96%) and encephalopathy (46.81%) were the common presenting features. The commonest causes of acute kidney dieses was hypovolemia (27.66 %) followed by Acute Glomerulonephritis was observed in 25.53%. Pregnancy Related Cause and sepsis was seen in 10.64% cases respectively. The mortality due to AKI was 10.63% in the present study. Conclusion: The acute renal failure requiring dialysis was seen commonly in young male, mostly belonging to urban area and presents with Oliguria, Edema and Encephalopathy. The most common cause for acute renal failure and mortality associated with it was Hypovolemia and Acute Glomerulonephritis. Key Words: Acute Renal Failure, dialysis, Clinical features, Outcome.
INTRODUCTION Acute kidney injury (AKI) is defined as a rapid (over hours to weeks) and usually reversible decline in glomerular filtration rate (GFR) that can occur either in the setting of previously normal renal function (“classical” AKI) or in a patient with pre-existing chronic kidney disease (acute-onchronic renal failure; ACRF).1-3 Acute renal failure (ARF), now increasingly referred to as “acute kidney injury” (AKI), is characterized by sudden (i.e., hours to days) impairment of kidney function. Descriptions of AKI date back to the ancient Greek period4, when the diagnosis was possible only by observing a reduction in urine volume. The modern day conception of AKI has evolved alongside developments in pathology and clinical biochemistry, which have permitted clinicopathologic correlations and early diagnosis5. Initial descriptions of AKI from the early 20th century centered around specific conditions, such as crush injuries6, war nephritis7, and falciparum malaria8. Sir William Osler in 1912 described several recognizable causes of AKI under the heading of “acute Bright’s disease,” including sepsis, pregnancy, burns, and toxins9. Early identification of high-risk patients would allow greater targeting of tailored interventions and more appropriate allocation of limited clinical resources10. Additionally, robust prognostic models would aid in the conduct of clinical trials by enriching the study population with individuals who are more likely to experience the clinical event of interest11,12.
MATERIALS AND METHODS The present hospital based retrospective cross-sectional study was done at department of medicine of Dr. Ulhas Patil Medical College and Hospital All the adult AKI patients who required haemodialysis and admitted during the January 2016 to December 2016 were enrolled in the study. The medical records of all patients admitted during the study period were studied. All patients of age 14 and above with AKI and have been dialyzed at least once during the study period were included. In the hospital patients of age 14 and above are considered as “adults” and admitted to the adult patient wards. Those patients who had dialysis for overdose of dialyzable drugs, those who were under the age of 14 or had incomplete or missing records were excluded. AKI was defined as an increase in SCr by 0.3 mg/dl within 48 h or a 50% increase in SCr from the baseline within 7 days according to the KDIGO criteria [ref2-16]. Patients were classified according to the KDIGO criteria as specified by stage 1, stage 2 and stage 3. The date of AKI onset was defined as the earliest day that the SCr change met the KDIGO criteria. The stage of AKI was determined using the peak SCr level after the date of AKI onset. Data on sociodemographic details, clinical features and causes associated with AKI were recorded on a prestructured proforma. The collected data was entered in Microsoft excel and was analysed and presented with appropriate tables and graphs.
RESULTS Table 1: Demographic distribution of study patients
It was observed that majority of the patients requiring dialysis with acute kidney disease were young with age less than 40 years of age. The proportion of male patients (59.57%) was more as compared to female patients (40.43%). It was seen that 70.21% patients were from urban area and remaining 29.79% were belonging form rural area.
Table 2: Distribution according to presenting symptoms
The most common presenting features were oligouria (80.85%), edema (65.96%) and encephalopathy (46.81%).
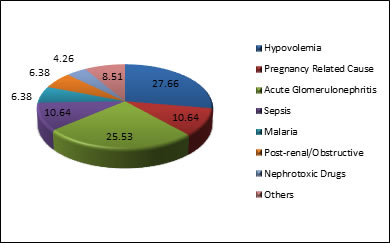
Table 3: Distribution according to Common Causes of dialysis requiring AKI
It was seen that the commonest causes of acute kidney dieses was hypovolemia (27.66 %) followed by Acute Glomerulonephritis was observed in 25.53%. Pregnancy Related Cause and sepsis was seen in 10.64% cases respectively.
Figure 1: Distribution according to Common Causes of dialysis requiring AKI
Table 4: Distribution of outcome according to specific cause of AKI
It was seen that there were total 5 deaths in the study patients in AKI. Out of them 3 were due to Hypovolemia, one was due to Acute Glomerulonephritis and one was due to Nephrotoxic Drugs. Thus the mortality due to AKI was 10.63% in the present study.
DISCUSSION The present study was conducted at the department of medicine with the aim to study the Clinical features and Outcome of patients suffering from Acute Renal Failure requiring dialysis. Thus total 47 cases were studied; admitted during the study duration with AKI and requiring dialysis. It was observed that majority of the patients requiring dialysis with acute kidney disease were young with age less than 40 years of age. Ibrahim et al13 observed that the mean age of patients with AKI was 36.7 ± 14.5 years, with more than two third being in the age group between 21 to 40 years. The proportion of male patients (59.57%) was more as compared to female patients (40.43%). Gender distribution observed by Ibrahim et al13 was nearly equal, with 50.3% being male. It was seen that 70.21% patients were from urban area and remaining 29.79% were belonging form rural area. Similar findings were also observed by Ibrahim et al13. Acute Kidney Injury (AKI) is an abrupt decline in kidney function and is a clinical condition that occurs in 10- 20% of hospital admissions and remains the most common reason for inpatient nephrology consultation14,15,16. Patients who develop AKI have higher rates of morbidity, mortality, and end-stage kidney disease17. The most common presenting features were oligouria (80.85%), edema (65.96%) and encephalopathy (46.81%). Similar findings were also reform Emen-Chioma18 and Bagshaw19 and Ibrahim et al13. It was seen that the commonest causes of acute kidney dieses was hypovolemia (27.66%) followed by Acute Glomerulonephritis was observed in 25.53%. Pregnancy Related Cause and sepsis was seen in 10.64% cases respectively. Severe preeclampsia, eclampsia, postpartum haemorrhage and puerperal sepsis wee the pregnancy related causes. In the study by Ibrahim et alref1 the commonest causes of AKI (22.5 %) was observed to be hypovolemia due to gastrointestinal loss (in the form of diarrhoea or vomiting) or blood loss. AGN and pregnancy related cause was seen in 21.9% and 18.5%. It was seen that there were total 5 deaths in the study patients in AKI. Out of them 3 were due to Hypovolemia, one was due to Acute Glomerulonephritis and one was due to Nephrotoxic Drugs. Thus the mortality due to AKI was 10.63% in the present study. Ibrahim et al13 observed the mortality rate of 29.1% in their study. The mortality observed in the study was much lower than the data from a global meta-analysis of studies done across the globe which has shown a pooled AKI-associated mortality rate 49.4 % for dialysis requiring AKI. The rate of AKI-associated mortality seems to be lower in developing countries and varies from 10% to 40%.20,21,22 In contrast to developing countries, very high mortality rates of AKI are reported from developed countries, ranging between 37% and 81%.23-27
CONCLUSION Thus we conclude that acute renal failure requiring dialysis was seen commonly in young male, mostly belonging to urban area and presents with Oliguria, Edema and Encephalopathy. The most common cause for acute renal failure and mortality associated with it was Hypovolemia and Acute Glomerulonephritis.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.