|
Table of Content Volume 12 Issue 2 - November 2019
Can we diagnose the ligament tear of ankle using X-RAY?
Roshan S1, Niveditha Pandey2*, Gautham Kamble3
1Associate Professor, Department of Anatomy, Kanachur Institute of Medical Sciences, Mangalore
2Associate Professor, Department of Anatomy, NC Medical College, Israna, Panipat, Haryana.
3Asistant Professor, department of Anatomy, Yenepoya Medical College.
Email: dr.shishirkumar091010@gmail.com
Abstract Ligaments of the ankle are one of the most frequently injured as we are bipeds and thus a lot of pressure is put on the bones that form the ankle and the ligaments that are under constant pressure to ascertain the tasks. One sixth of the static load of the leg is carried by the fibula at the tibiofibular joint. These require a high degree of stability which is determined by the passive and dynamic factors. The passive stability depends on the contour of the articular surfaces, the integrity of the collateral ligaments, the integrity of the distal tibiofibular ligaments, the reticular system around the ankle and the crossing and attached tendon tunnels. The study puts in an effort to find whether the ligaments injury can be diagnosed on a simple X-Ray?
Key Word:
INTRODUCTION
Ligaments of the ankle are one of the most frequently injured as we are bipeds and thus a lot of pressure is put on the bones that form the ankle and the ligaments that are under constant pressure to ascertain the tasks. One sixth of the static load of the leg is carried by the fibula at the tibiofibular joint1. These require a high degree of stability which is determined by the passive and dynamic factors2. The passive stability depends on the contour of the articular surfaces, the integrity of the collateral ligaments, the integrity of the distal tibiofibular ligaments, the reticular system around the ankle and the crossing and attached tendon tunnels5,6,7. The lateral ligament is injured more often when compared to medial. A sprained ankle results due to tear of anterior talofibular and calcaneofibular ligaments when the foot is twisted in lateral direction. In forcible eversion of the foot the deltoid ligament may be torn. At times the deltoid ligament pulls the medial malleolus thereby causing avulsion fracture of the malleolus. Potts fracture occurs when the foot is caught in the rabbit hole in the ground and the foot is forcibly everted. In this condition at first there is an oblique fracture of shaft and lateral malleolus of fibula. The strong eversion pull on the deltoid ligament causes transverse fracture of medial malleolus. If the tibia is carried anteriorly, the posterior margin of the distal end of the tibia is also broken by the talus producing a trimalleolar fracture8,9.Magnetic resonance (MR) imaging has opened new horizons in the diagnosis and treatment of many musculoskeletal diseases of the ankle and foot. It demonstrates abnormalities in the bones and soft tissues before they become evident at other imaging modalities. But in a nation like ours the MRI is not there in a village set up and cost factor plays a major role. It is important to use simple X-Rays to diagnose the same.
AIMS AND OBJECTIVES
To study the normal X-Rays and try to measure normal parameters so as to be useful in diagnosing the ligament tears when there are no fractures evident on X-Rays in the west coast population.
MATERIALS AND METHODS
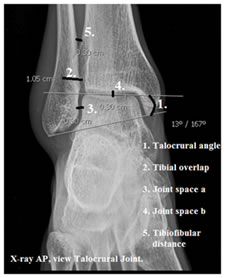
This study was done in the Department of Anatomy, Srinivasa Medical College, Mangalore. This study was done from March 2014 to February 2016. One hundred X-Rays were collected from the Department of Radiology and the study was done. The following were measured.
RESULTS
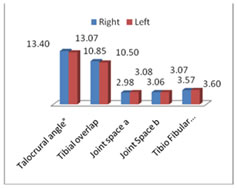 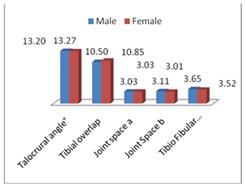
Table 1: Left Vs Right Table 2: Male Vs Female
DISCUSSION
It is important to use whatever is available and try to come to a diagnosis and that’s where the study of the basic sciences comes in handy. Use of the basic knowledge to come to definitive diagnosis is what is meant to be a good doctor instead of heavily relying on the advances in the field of sciences. Patil MS et al.10 in 2012 in their study on anthropometric measurements of ankle mortise for evaluating mortise fracture reductions with an aim to develop contoured implants measured the talocrural angle, tibiofibular clear space, tibiofibular overlap and compared joint clear space at two places. Anteroposterior radiographs, of both ankles in 20 adult individuals formed the material. They agreed that the talocrural angle of two ankles of a given individual does not vary by more than 2 degrees. Tibiofibular clear space on Anteroposterior radiographs measured a mean value of 2.4 mm with a standard deviation of 1.3 mm. Tibiofibular overlap on Anteroposterior radiographs was measured as 11.2 mm with a standard deviation of 4.4 mm. Joint spaces at two levels were almost equal. Chen Yan-Xi et al.11 in 2011 on a study of three-dimensional morphological characteristics measurement of ankle joint based on computed tomography image post-processing, commented that the mean talocrural angle (10.01±0.38)° was measured to be 10.1 degrees with a standard deviation of 0.38 degrees Tibiofibular clear space mean measurements were 2.78 mm, with a standard deviation of 0.19 mm. There was no significant correlation to gender, height and weight (P >0.05) in 100 cases, (50 males and 50 females). This study helps to firmly put in a foundation towards forming measurement standards so as to be helpful in diagnosing the ligament injuries.
CONCLUSION
A firm foundation is put in forming measurement standards so as to be helpful in diagnosing the ligament injuries.
REFERENCES:
- Lambert KL. The weight bearing function of the fibula. A strain gauge study. J Bone Joint Surg Am. 1976; 53 (3): 507.
- McCullough CJ, Burge PD. Rotary stability of the load bearing ankle. An experimental study. J Bone Joint Surg Br. 1980; 62(4): 460.
- Inman VT. The joints of the ankle. Baltimore: Williams and Wilkins 1976: 19, 26, 27, 31, 37, 70 – 73.
- Lundberg A, Nemeth G, Svensson O K, Selvik G. The axis of rotation of the ankle joint. J Bone Jt Surg. 1989; 71B: 94 – 99.
- Sammarco J. Biomechaninics of the ankle. Surface velocity and instant center for rotation in sagittal plane. Am J Sports Med. 1977; 5: 231 – 234.
- Jend H H, Ney R, Heller M. Evaluation of tibiofibular motion under load conditions by computed tomography. J Orthop Res. 1985; 3: 418 – 423.
- MacConaill MA, Basmajian JV. Muscles and Movements. A Basis for Human Kinesiology. Baltimore: Williams and Wilkins. 1969; 78, 79.
- Barnett CH, Napier JR. The axis of rotation of the ankle joint in man. Its influence upon the form of the talus and the mobility of the fibula. Anat. 1952; 86: 1.
- Inderbir singh. Squatting facets on the talus and tibia in Indians. J Anat. 1959; 93: 540.
- M.S. Patil, S.M.G. Raza, Md. Nayeem Ali. Anthropometric measurements of ankle mortise for evaluating mortise fracture reductions with an aim to develop contoured implants. Al Ameen J Med Sci 2012; 5(4): 381-387.
- Chen Yan-xi, Lu Xiao-ling, Bi Gang, Yu Xiao, Hao Yi-li, Zhang Kun, Zou Li-ling, Mei Jiong, Yu Guang-rong. Three-dimensional morphological characteristics measurement of ankle joint based on computed tomography image post-processing. Chin Med J. 2011; 124(23): 3912-3918.
|
|
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.