 Home
Home|
Table of Content Volume 12 Issue 3 - December 2019
Ananthi V1*, Rajkumar D2, Muniappan V3
1Tutor, 2Dean, 3Professor and HOD, Department of Anatomy, Rajah Muthiah Medical College, Annamalai University, Chidambaram. Email: ananthisricharan@gmail.com
Abstract Background: Placenta is a fetomaternal organ, acts as a mirror and reflects the fetal growth in utero. Umblical cord is a connecting link between fetus and placenta. Our present study aimed to find the mode of insertion of umblical cord and various placental shapes in natural conception and in assisted reproduction. Materials and Methods:30 Placentas of natural conception and 30 placentas with 42 umblical cords (12 cases of Twins, 18 cases of singleton) of assisted reproduction were collected from obstetrics and Gynaecology department, Rajah Muthiah Medical College and Hospital and from Private Fertility centre in and around Chidambaram. Human ethical committee clearance was obtained before sample collection. Shape of placenta and mode of insertion of umblical cord were examined and noted. Umblical cord diameter was measured using measuring tape and compass. Results and Discussion: Diameter of umblical cord was 1.2 cm in natural conception, 0.89 cm in assisted reproduction. Irregular shape of placenta was increased in assisted reproduction and velamentous cord insertion was also increased in assisted reproduction. These results would be useful in Neonatologists who handle newborns of assisted reproductive mothers. Key Words: Velamentous insertion, Diameter, Shape of placenta, Eccentric insertion
INTRODUCTION The placenta is a vital organ, which reflects the internal status of fetus in utero. It has two components fetal portion which is formed by villous chorion, maternal portion formed by decidua basalis, the part of uterine endometrium.1 Umblical cord is the connecting cable and link between the fetus and placenta. The embryo remains attached to the trophoblast by extra embryonic mesoderm in into which the coelom does not extend. This extra embryonic mesoderm forms the connecting stalk. As a result of embryonic end of connecting stalk comes to lie on the ventral surface of embryo. It is attached in the region of umblical opening.2 The umblical cord consists of an outer covering of flattened amniotic epithelium, containing Wharton’s jelly (an interior mass of mesoderm) with two umblical arteries and one umblical vein. Initially there are two arteries and two veins. Later right vein disappears. The umblical cord normally insert to the central portion of placenta, well away from placental edge3,4, it’s considered as central insertion of cord. If the umblical cord is inserted within 2 cm from the placental edge, it is considered as marginal insertion.5,6 Grossly visible branching of the umbilical vessels before their insertion onto the placental surface is known as furcated placenta. Human placenta is defined as discoidal organ (in contrast to the other shapes eg. zonary, bidiscodal, diffuse etc).After delivery of the fetus, the placenta becomes separated from the uterine wall and together with so called ‘membranes’ is expelled as “after birth” 7. Placenta shape, size and insertion of cord vary widely between pregnancies. The placental shape is usually round or oval. However it may be irregular, bilobate or multilobate. Irregular placental shape has been associated with low birth weight, altered feto placental ratio, as it may show the altered placental function in utero 8. Placenta utilizes the 1/3 of oxygen and glucose that are supplied to maternal blood, protein synthesis rate was higher in placenta when compared to liver9. The probability of identifying congenital anomalies will be higher with meticulous umblical cord examination in the earlier period of gestation 10. Assisted Reproduction: Assisted Reproduction is a technique where gametes are manipulated artificially, fertilized embryo can be reinserted into mother’s uterus. Assisted Reproductive Technique (ART) is an invaluable gift to infertile couple those who are exhausted by taking various treatments and failed it. There are some fall outs in ART because of artificial manipulation of gametes. Intracytoplasmic sperm injection [ICSI] is a technique where the deposition of single spermatozoon directly into cytoplasm of oocyte, thus bypassing the zona pellucida and oolemma. Our present study aimed to analyze the variations in the placental shape, mode of insertion of umblical cord, diameter of umblical cord in assisted reproduction and its clinical significance in Indian population.
MATERIALS AND METHODS 30 placentas of natural conception and 30 placentas with 42 umblical cords (out of 30, 12 cases are dichoionic diamniotic twins and 18 cases are singleton ) of assisted reproduction were collected from OG Department, Rajah Muthiah Medical College and Hospital and from private fertility centre in and around Chidambaram. Human ethical committee clearance was obtained before sample collection. Placentas were washed in running tap water to remove the blood clots. Completeness of membranes was examined, shape of placenta was observed and diameter of umblical cord was measured using measuring tape and compass. Mode of insertion of umblical cord was observed on fetal surface of placenta.
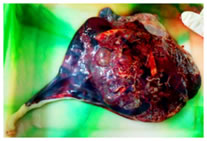
RESULTS Changes in the development and site of insertion of umblical cord can cause problems which have the potential to affect the maternal and fetal growth and development [11-13]. Diameter of cord, various placental shapes and mode of insertion of umblical cord of natural conception and assisted reproduction were noted and tabulated. Furcated placenta was noted in 2 cases of assisted reproduction (fig 1).
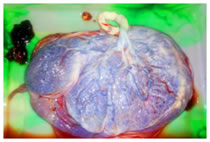
Figure 1: Furcated placenta Figure 2: Velamentous insertion of umblical cor Figure 3: placenta with accessory lobe Figure 4: Succenturiate placenta with cyst
Statistical analysis was performed for analyzing the diameter of umbilical cord using SPSS. The data obtained from the study were compiled and expressed as mean ± standard deviation. Mann-Whitney test was performed. Two tailed ‘t’ test were done. Z value and P values are alto tabulated. P value of < 0.05 was taken as significant.
Table 1: Various shapes of placenta in natural conception and in assisted reproduction
Table 2: Mode of insertion of umblical cord in natural conception and assisted reproduction
DISCUSSION The deoxygenated fetal blood leaves the fetus through two umblical arteries that passes through umblical cord. When they reach the fetal surface of placenta, the vessel divided into branches and enters the chorionic villi. The oxygenated blood returns to the fetus through venules and veins in chorionic villi that forms umblical vein.“Trophotrophism” is a process in which the chorionic frondosum or early placenta moves with advancing gestation to get a better supply from vascularised area.14 The conceptus once reaches the blastocyst stage, it is able to implant. Once it formed as blastocyst, it become asymmetrical and internal cells forms compact inner cell mass that remain in contact only with the part of outer polar region. ART procedures may interfere in some ways with polar trophoblast differentiation. In Donald N.Disalvo et al 15, sonographic studies of 46 pregnancies, he found the central insertion of cord in 70.37% cases, marginal mode of insertion in 22.22% cases, velamentous mode of insertion in 7.41% cases.In Sepulveda et al 16 study, they found central mode of insertion of cord in 93.8%cases, marginal mode of insertion in 5.21% cases and velamentous insertion in 0.96% cases using colour doppler ultrasound study. According to Manikanda Reddy et al 17, 75.45% of cases were central mode of insertion, 16.36% of cases were marginal insertion of cord, 7.27% of cases were furcated placentas and 0.9% of cases were velamentous type of insertion. In Gavrill et al 18 study, abnormal shape of placenta significantly increased in assisted reproduction when compared to control group. There was a significant difference in the insertion of cord in ART when compared to natural conception. In our present study central mode of insertion of cord was found in 56.66% cases, eccentric mode of insertion of cord was found in 40% cases and marginal mode of insertion of cord was found in 3.33 % cases in natural conception (table 2). In ART pregnancies, central mode of insertion was found in 57.14% cases, eccentric mode of insertion of cord was found in 16.66% cases, marginal mode of insertion of cord was found in 16.66% cases and velamentous mode of insertion of cord was found in 9.52% cases(fig 2, table2). Velamentous insertion of cord was significantly increased in assisted reproduction. Our present study results were in concurrent with the Gavrill et al study. This velamentous insertion is associated with low birth weight, growth retardation, low APGAR score, abnormal fetal heart patterns and congenital anomalies like oesophageal atresia, obstructive uropathies, congenital hip dislocation, assymmetrical head shape, spina bifida, VSD, single umblical artery, bilobed placenta.19,20 In Ragunath et al21 study, placenta in most of cases was round in 93.7%cases, oval in 7% cases. But accessory lobe was not found. In present study shape of the placenta was round in 70% cases, oval in 23.37% cases and irregular in 14.28% cases of natural conception. There was a significant increase in irregular shape of placenta in assisted reproduction (table 1). Accessory lobe was found in 13.33 % (4/30) cases of assisted reproduction (fig 3). There was a cyst on the fetal surface of placenta in 6.66 % (2/30) cases (fig 4). Abnormal shape has been associated with increased intra uterine fetal death, extreme preterm delivery and fetal growth restriction 22.In Annapurna et al 23 study, mid thickness of umblical cord was 2.1 to 3.5 cm in majority of cases. According kouvalainen et al 24, average diameter of umblical cord was 1.5 cm. In present study mid thickness of cord was 1.2 cm in natural conception, 0.89 cm in assisted reproduction. Our present study results were in concordance with previous study. There was a significant reduction in diameter of umblical cord in assisted reproduction. So compression of vessels within cord may occur, which may cause fetal growth retardation, small for gestation age. Over all there was a significant reduction in diameter of cord in ART. Irregular shape of placenta was increased in ART and also velamentous cord insertion was increased in ART. These changes may affect the fetal growth and development indirectly. These data would be useful for neonatologists who handle newborn of ART mothers.
CONCLUSION We conclude that there was significant changes in the placental shapes, mode of insertion of umbilical cord in assisted reproduction when compared to natural conception .These results would affect the fetal growth and development indirectly. These results will be useful for obstetricians and gynecologists who handle the infertile cases.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.