 Home
Home
|
Table of Content Volume 17 Issue 2 - February 2021
Histogenesis of human fetal pancreas
Swati Patil1, Avinash D Shewale2*, Rohini Karambelkar3
1Associate professor, 3Professor and HOD, Department of Anatomy, PIMS and R, Islampur, INDIA. 2Associate professor, Dept of Anatomy, BKLWRMC Sawarde, Chiplun, INDIA. Email: shewaleavi11@gmail.com Abstract Background: Pancreas is the digestive gland with exocrine and endocrine responsible for glucose homeostasis. Now a days clinicians are making an attempt to treat patients of insulin dependent diabetes mellitus and pancreatic carcinomas by transplantation of fetal pancreas. So the clinical studies require complete knowledge of development and morphology of pancreas. Present study was conducted to see changes occurring in pancreas in fetuses of different gestational ages. The study showed that acini, islets and ducts of the gland develop from primitive tubules and establish their separate identity. Key words: islets of Langerhans, histogenesis, pancreas
INTRODUCTION Pancreas develops from two endodermal evaginations namely dorsal and ventral pancreatic buds1. The exocrine pancreas consists of acinar cells which are responsible for secretion of enzymes of digestion, pancreatic fluids. Pancreatic islets of Langerhans are ovoid clusters of polyhedral cells situated more in tail region of pancreas. Depending upon immunostaining properties and morphology, the cells in the islets are divided into different types: A, B, D, E and F cells. A cells secrete glucagon, B cells secrete insulin, D cells secrete somatostatin, E cells secrete gherlin, F cells secrete pancreatic polypeptide.2 There is persistent need for gaining insight into the natural history and embryology of pancreatic islets because the pancreatic beta cell may be a primary site of pathology in diabetes and the numbers of functioning beta cells affect the initiation or outcome of disease4. The present study aim to carry out a light microscopic study in order to determine the sequence of histologic differentiation of exocrine and endocrine components of pancreas.
MATERIALS AND METHODS In the present study about 30 fetuses, ranging from 12-40 weeks with no obvious congenital anomaly were obtained from the department of Obstetrics & Gynaecology of Armed Forces Medical College. These fetuses included spontaneous abortions, stillborn, preterm babies and also a few autopsy specimens. Fetuses were arranged in five gestational age groups with 6 weeks interval. The fetuses were immediately fixed in 10% formalin. Pancreas was then dissected and fixed in 10% formalin for 48-72 hours, and then processed for paraffin sections of 5mm thickness. The sections were stained for light microscopic study with haematoxylin and eosin, Mallory’s phosphotungstic acid and Gordon and Sweet stain.
OBSERVATIONS Histology of pancreas was studied by examining slides after staining with Haematoxylin and Eosin and observed under low and high-power magnification of a light microscope. Histological observations made are as follows:
Figure 1: Dissecting foetuses to obtain pancreas
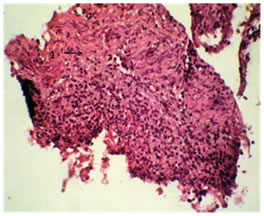
12-to-13-week stage of pancreas: In 12-to-13-week fetuses, it was observed that, branched tubule with wide lumen was embedded in the mesenchymal tissue. Budding was seen at the ends of these tubules forming primitive acini and islets. Parenchyma began to organize into lobes and lobules. Islets, the endocrine component were small and spherical.
Figure 2: ( X100) Microphotograph of 12th week pancreas. H and E Stain showing 1. mesenchymal tissue
13.1-18-week stage of pancreas:
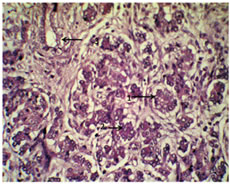
Lobes and lobules were more established in parenchyma. Size of islets had increased. Cells in islets were more evenly distributed. Some undifferentiated mesenchymal tissues were seen. 18.1-24-week stage of pancreas: Parenchyma was well organized into lobes and lobules. Tubules were differentiated into ducts which may be interlobular and intralobular. Islets were increased in size. They were well encapsulated and cells in the islets were closely packed. Islets were better differentiated with Gordon and Sweet stain and Mallory’s phosphotungstic acid.
Figure 3: ( X400 ) Microphotograph of 22ndweek pancreas. H and E Stain showing 1. well encapsulated islets, 2.acius, 3.intralobular duct
DISCUSSION In the present study, while studying the development of pancreas in antenatal period, different morphological and histological parameters of pancreas are considered. The findings of the present study were compared with that of other researchers and are as under:
According to study conducted by Manupati S., at 8-10 weeks parenchyma began to organize into lobes and lobules with abundant mesenchymal tissue. In 16-18 weeks, they were separated by connective tissue5. Gupta et al. observed that, in early weeks of fetal maturation, primitive tubules exhibit budding of cells which differentiate into acini, islets or ducts. At 12 weeks, organization of parenchyma began to form lobes and lobules, at 14-15 weeks the organization was well defined6. In the present study, it was seen that at 12-13 weeks parenchyma began to organize into lobes and lobules. Budding at the ends of branched tubules resulting in the formation of primitive acini. In 13-18 weeks, more branched tubules with more established lobes and lobules were seen. In 18-24 weeks, it was found that parenchyma was well organized into lobes and lobules.
In early weeks of maturation, parenchyma composed of undifferentiated mesenchymal tissue surrounded around lobes and lobules. This observation of our present study matches with that carried out by previous researchers.
Study by Gupta et al. states that, by the 18-24 weeks, ducts were differentiated into intralobular and interlobular. Parenchyma consisted of collection of branched tubules lined by cuboidal cells which proliferated to form primitive islets, acini and ducts6. Similar findings were observed in the present study.
Hamilton and Boyd stated that, in the third month of fetal life, the islets of Langerhans develop from the collecting tubules to form isolated groups of cells in which secretory granules can be identified. By the fourth month the islet tissue constitutes approximately a third of the total pancreatic mass7. According to Skandalakis, two populations of endodermal cells develop: those that form ducts and acini, and those that form islet cells. Ducts and acini form first, but islet primordial bud off ducts as soon as they are formed8. In the present study it was found that at 12-13 weeks of age, islets were small and spherical. As the age of fetus increased, size and number of islets also increased.
CONCLUSION The findings were in concurrence with studies done on the subject by earlier workers. Findings were in agreement with what has been noted by workers on the subject earlier. There was no local variation in the normal histogenesis observed during the present study and all findings were comparable with earlier studies. It was noted that fetal pancreas of 22-24 weeks are suitable donor for transplantation, but it also requires more detailed biochemical and ultrastructural analysis for accurate staging. Thus successful fetal pancreas transplant requires the knowledge of its development, morphology, insulin content and its response to glucose at various stages of islet genesis. An understanding of normal histogenesis of pancreas along with some common variations possible is a stepping stone towards this correlation. However a study group involving a larger sample size and the use of electron microscopy with special staining techniques will add to this understanding and aid in the early definitive diagnosis of certain pancreatic diseases.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Community Medicine (Print ISSN: 2579-0862) (Online ISSN: 2636-4743) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.