 Home
Home
|
Table of Content - Volume 19 Issue 1 - July 2021
The relationship between the weight of the placenta and birth weight of neonate in Konaseema area, east Godavari, Andhra Pradesh
M Sudhakara Rao¹, G Sailaja2*, K Deepika3
1Assistant Professor, Department of Anatomy, Konaseema institute of medical sciences, Amalapuram, Andhra Pradesh, INDIA. 2Assistant Professor, Department of Anatomy, Rangaraya Medical College, Kakinada, Andhra Pradesh. INDIA. Email: joysaila@gmail.com
Abstract Background: Survival and growth of foetus is essentially dependent on formation, full development and function of the placenta. It is mirror which reflects the intrauterine status of the foetus. The aim of this study is to determine the well being of the baby in relation with the weight of placenta, the present study is to correlate the weight of the placenta with the weight of foetus. Reduction in placental weight and size has been associated with reduced foetal growth and also risk of foetal growth restriction. Keywords: Placenta; Placental Weight; Foetal Weight;
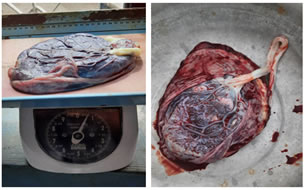
INTRODUCTION PLACENTA is a vital organ for maintaining normal pregnancy and promotes foetal development. It is a dynamic organ which unique in its development and functions. It is the only organ in the body which is derived from two separate individuals, the mother and the foetus. Being such a vital organ, it has evoked great interest among the anatomists, pathologists and obstetricians to study this organ in details in normal pregnancies as well as in various pregnancy induced abnormalities. A morphologically normal placenta reflects a healthy foetal status and vice versa. Any structural abnormality of the placenta would adversely affect the foetus resulting in low birth weight like either pathological conditions. The well being of the foetus is affected by many factors but a healthy placenta is the single most important factor in producing a healthy baby (Van den Broek et al., 2005; Kliman 1997). The placenta begins to form at about the seventh day after fertilization when the first cell layer of cytotrophoblast is observed. During pregnancy, a range of problems may occur that could lead to foetal abnormalities and death. Although these problems could arise from a variety of sources including chromosome and genetic disorders of the foetus (e.g. Down’s syndrome), maternal illness or behaviour (e.g. Pre-eclampsia, smoking), environmental factors (e.g. radiation) the most important of them all is placental abnormalities (Yetter, 1998). Information regarding weight of Placenta may be important to the care of both mother and infant (Yetter, 1998). The placenta is a complex multifunctional organ of mainly foetal origin with pleiotropic roles during foetal growth. It has a portion derived from the developing embryo and a maternal portion formed by the modification of the uterine lining of the mother (Yetter, 1998). During the gestational period, it provides nutrition, gas exchange, waste removal, endocrine, immune support and a special circulation system (Pijnenborg et al., 1983) to the developing foetus. It separates the maternal and foetal circulation, with which it is in contact through different surfaces, i.e., the syncytiotrophoblast exposes the placenta to the maternal circulation and the foetal vascular endothelium is in contact with foetal blood (Desoye and Haugel-de, 2007). The placenta comprises a large number of functional units called villi which contains branched terminals of the foetal circulation allowing transfer of metabolic products. The placenta is blue- red in colour and discoid in shape, 15- 22 cm in diameter, 2- 4 cm thick, weighs 400- 600g. (Yetter, 1998). It is classified as chorio- allantoic since it is vascularized by vessels homologous with allantoic vessels of lower mammals; haemo-chorial because of the nature of the placenta membranes; villous because of their villi (Foidart et al., 1992) It has a maternal surface that is divided into lobules or cotyledons with irregular grooves or clefts; the foetal surface is smooth, shiny, translucent and covered in amniotic membrane (Borton, 2006). The foetal surface of a full term placenta is shiny, grey and consists of large opaque blood vessels distributed on the dense opalescent surface of the thickened chorion. The maternal surface has the dark red colour of venous blood. The placenta uses about 1/3 of all the oxygen and glucose supplied to the maternal blood and the rate of protein synthesis is higher in the placenta than the liver (Kaplan, 1995). It is estimated that more than 7.6 million perinatal deaths occur each year world wide; 4.3 million of these are foetal deaths (Sornes, 2000). Ninety-eight percent of perinatal deaths have been said to take place in developing countries, and the perinatal mortality rate is estimated to exceed 55 per 1000 births, which is five times higher than in developed countries (Salafia and Vintziloes, 1999). Several studies have been conducted in the developed countries and Asia which have suggested that placenta indices have a significant role in foetal growth in terms of weight, body length, and cord length (Lurie et al., 1999; Salafia and Vintziloes, 1999). Currently very little is known about the incidence of fetal deaths resulting from placenta malformation therefore the present study was designed to provide some information on the relation between the placental weight and foetal weight. The present study shall therefore be undertaken to record data on weight of the placenta and its correlation with foetal weight in tertiary care hospitals of konaseema area due to lack of this type of study in this area. MATERIALS AND METHODS SPECIMEN COLLECTION AND PREPARATION Two hundred and eight placentae with their attached umbilical cords from the uncomplicated pregnant women of age group between 20 and 35 years were collected from the obstetrics and gynecology department of konaseema institute of medical sciences and research foundation and other hospitals in konaseema area. In all cases, after separating the baby from the umbilical cord, the specimens were tagged with numbers that corresponded with the numbers indicated in the data of the perinatal outcomes and placed in a container of 10% formalin. Samples were picked up and washed clean of blood and stored again in a solution of 0.5% formaldehyde in saline for further detailed examination and measurements. The birth weight of normal babies recorded from the parturition register of above mentioned hospitals .Patients gave informed consent in the labour room before being included in the present study the study was approved by the Institutional ethical clearance committee and head of the obstetrics and gynecology department. After collection of specimen’s placental weight and foetal weight were measured.Weight of placenta was determined by an electronic balance ( ATOM electronic compact scale. 0.000 grams to 2000 grams) and recorded against its specific number. The birth weight obtained from the centers and categorized them into two as those with birth weight less than 2.5 kgs ( low birth weight) and those with greater than or equal to 2.5 kgs ( normal birth weight). INCLUSION CRITERIA: Women with normal and uncomplicated pregnancy.-consecutive singleton normal deliveries, cesarean sections and mothers of age group 20-35 years EXCLUSION CRITERIA: Women with complicated and abnormal pregnancy congenital anomaliesencies.-maternal diseases like diabetes mellitus ,hypertension, anemia, multiple pregnancies TYPE OF STUDY: Cross sectional study. STATISTICAL ANALYSIS: All the collected data was tabulated in excel spreadsheet, processed and analysed, . placental weight, were expressed in mean standard deviation and correlated with fetal weight using correlation coefficient r value, student t test and pearsons correlation. p value less than 0.05 will be considered as statistically significant.
RESULTS Table 1: Mean±SD of placental parameter
Table 2: Range of placental parameters
Table 3: Correlation coefficient
Figure 1 Figure 2 Figure 3 Figure 4
DISCUSSION The weight of the placenta is used in the determination of the foeto-placental ratio. The weight of the placenta gives an idea of the amount of substance that is exchanged between the mother and the foetus. The mean placenta weight was 458.25g+\-99.71 (SD ) with a range of 289 to 754 in fetal weight >2.5kg and540.09+\-83.69(SD) with range of377 to 815 in fetal weight >2.5kg(Table.1and2). The weight of the placenta was found to have a significant positive correlation with the weight of the baby (r = 0.464, p<0.01)(Table.3). Luz (2001), in a similar experiment found the mean placental weight to be 537g (SD=96g). Lurie et al., (1999) also found the mean placental weight to be 613.0±123.8g with a range of 319- 1266g whilst Lo et al., (2002) had the mean placental weight to be 646.2±0.3g. However, (Borton, 2006) put the weight of the term placenta between 400- 600g, whilst (Yetter, 1998) put the term placenta to be about 470g. Comparing the mean placental weight obtained in this experiment to those obtained above, it was realised that the mean placental weight obtained by Yetter, (1998) was too low to be taken as the mean while that of Luz was more to the mean obtained in the present study. In contrast, Lurie et al. (1999) mean placental weight was found to be higher than the one obtained here. Since Borton gave a range for the term placental weight, the mean placental weight obtained fell within this range even though the range here was 289-815gm. This indicates that the mean placenta weight differs from place to place and may be due to so many factors such as nutrition, genetics, gestational age, maternal size, etc It was found that the placental weight correlates significantly with the weight of the baby and for every 1g increase in the placental weight, the foetal weight increases by 2g and this corresponds to (Luz, 2001) who found that for every 1g increase in placental weight, the foetal weight increases by 1.98g. Since the weight of the placenta correlated positively with the fetal weight , it then implies that, factors which directly affect the weight of the baby will indirectly affect the weight of the placenta. Such factors could include nutrition, maternal size, maternal haemoglobin gain, altitude, paternal factors, maternal and paternal genetics, gestational age, maternal diabetes mellitus, etc. According to (Van den Broek et al., 2005), unfixed placentae that weigh more than 600g are pathologic, but more important may be the placenta/foetal ratio. Chronic low uteroplacental blood flow is the most frequent cause of small placentae, but often the foetal weight is affected, so the ratio may be normal. The cause of enlargement may be unknown, but it is often revealed if the following are considered: overt or latent maternal diabetes, maternal anaemia, maternal–foetal blood group incompatibility, maternal–foetal transfusion, chronic intrauterine infection (syphilis), foetal malformations (especially of the lung), the twin transfusion syndrome, congenital neoplasms (e.g., neuroblastoma, teratoma, and chorangiomas) and alpha- thalassaemia. Some of these factors may be responsible for the differences between the placental weight obtained in the present study and those obtained by Salafia and Vintziloes (1999).
CONCLUSION The study on placenta is of great importance because this is the key point from where information about the fetus can begained. From this study it can be concluded that, in low birth weight baby all the placental parameter like its weight, its surface area, no of cotyledons etc are comparatively lower than the placenta of normal baby. So this theorem can be applied in detection of low birth weight before delivery through advanced diagnostic procedures like ultrasound, colour Doppler imaging. Also measures can be taken to reduce low birth weight child delivery, associated with its complications and thereby reducing infant mortality rate. There was a strong relationship between the placenta and the foetus suggesting that the well being of the foetus is highly dependent on the placenta since it serves as a link between the mother and the developing foetus for nutritional support, excretory functions as well as immunological and hormonal support. Large placentae provide a large surface area for the exchange of substances from the mother to the foetus resulting in high foetal weight, The best indicator of foetal weight is placental weight.. Critical examination of the placenta and umbilical cord immediately after delivery should be used to determine the well being of the baby.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.