 Home
Home
|
Table of Content - Volume 20 Issue 1 - October 2021
Size of lumbar vertebral canal and body: A correlative study of measurements in plain radiographs and dried bones
Asmita Sachin Jadhav1, Sachin B Jadhav2*, Anupama S Katti3, Rajani A Joshi4
{1,3Associate Professor, 4Professor & HOD, Department of Anatomy} {2Associate Professor, Department of Community Medicine} Government Medical College, Miraj, Maharashtra, INDIA. Email: dr_latesh@rediffmail.com
Abstract Background: The vertebral column bears the weight of trunk and upper limbs and transmits it to the lower limbs Low back pain is a common clinical problem. Stenosis of the lumbar canal causing nerve root compression is of great interest to the medical practitioner. Various anatomic studies have been conducted in different ethnic groups either by using specimens, radiographs or other methods so as to determine the normal limits of lumbar spine that will serve as baseline data. The present aims to study the normal dimensions of lumbar spinal canal and lumbar vertebral body taken on dry lumbar vertebrae and to correlate them with the measurements taken on radiographs of asymptomatic individuals. For the present study, two hundred normal plain radiographs and sixty four sets of normal lumbar vertebrae were studied.The transverse diameter of spinal canal, vertebral body and anteroposterior diameter of vertebral body were showing an increasing trend from L1 to L5 while anteroposterior diameter of spinal canal showed a gradual decrease. However the canal body ratio remained constant. The measurements from the osteological group were lower than the radiological group.The measurements also showed regional, gender variations, thus emphasizing the need to continuing such work so as to determine the normal dimensions in different regions. Key words: osteological, radiological, spinal index of jones,canal body ratio.
INTRODUCTION In man, the vertebral column supports the weight of the trunk and upper limbs, and also sustains much of the weight of burdens borne upon these parts of the body. The lumbar spine is sturdy and resilient however it is subjected to high degree of stress and load, that may cause many problems resulting in pain. The lumbar part of vertebral canal houses the conus medullaris and the cauda equina within a dural sac. The bony wall of the canal is unyielding and therefore an abnormal spinal canal stenosis at this level may lead to compression of the nerve roots. This leads to various symptoms from backache to various neurological manifestations. Narrowing of spinal canal may be congenital or acquired. In 1803, narrowing of the vertebral canal produced by abnormal curvature of the spine was first reported by Portal.1 Enlargement of spinal canal may be due to intraspinal tumour. Enlargement of vertebral body may occur due to non -weight bearing in conditions like paralysis, fibrous dysplasia etc. or may be due to congenital enlargement.2 Thus it is very important to study the dimensions of lumbar vertebrae. Studies by Anderson(1883),3 Cunningham(1886),4 Huizinga et al. (1951)5 etc have already established the importance of measurement of lumbar vertebrae by studying the lumbar vertebrae. Similarly, studies by Elseberg et al. (1934),6 Hinck et al. (1966)7 have also established the importance of measurements of lumbar vertebrae by the the use of roentgenogram. The present study aims to study the normal dimensions of lumbar spinal canal and lumbar vertebral body taken on dry lumbar vertebrae and to correlate them with the measurements taken on radiographs of asymptomatic individuals in Western Maharashtra population
MATERIALS AND METHODS STUDY –I (RADIOLOGICAL STUDY) For present study, only normal plain anteroposterior and lateral radiographs of lumbar spine of hundred adult male and female each of Western Maharashtra were utilized. These radiographs were of known sex and of known age group (between twenty-five and fifty years of age). The radiographs of both sexes had been taken in lying down position with an anode- film distance of one meter, cantered on L3. The measurements were made by using vernier caliper and were recorded to the nearest tenth of a milli meter. The following measurements were obtained from anteroposterior radiographs of lumbar spine. The Transverse Diameter of spinal canal/Interpedicular Distance: This corresponds to transverse diameter of spinal canal and was obtained by The Transverse Diameter of Vertebral Body: This was taken as the mid vertebral distance between the points on lateral borders of vertebral body shadow. Following measurements were obtained from lateral radiographs of lumbar spine: The Anteroposterior diameter of spinal canal: This was measured as the distance between the posterior border of the vertebral body shadow and shadow of spinolaminal junction of the same vertebra.8 The Anteroposterior diameter of vertebral body: This was taken as the mid vertebral distance between the points on anterior border and posterior border of the vertebral body shadow. STUDY – II (OSTEOLOGICAL STUDY) Three hundred and twenty lumbar vertebrae (sixty-four complete sets of lumbar spine) aged between twenty five and fifty years. Care was taken that Only those specimens which appeared normal were studied. Various measurements were taken by using vernier calliper and were recorded to the nearest tenth of a millimeter. Following measurements were taken: The Transverse Diameter of spinal canal: This was taken as the minimum distance between the medial surfaces of the roots of the vertebral arch of a given vertebra. The Transverse Diameter of Vertebral Body: This was measured as the minimum transverse distance across vertebral body, which is at the mid vertebral level. The Anteroposterior diameter of spinal canal: This was taken as the distance between the posterior margin of the body and the midpoint of the vertebral arch. The Anteroposterior diameter of vertebral body: It was measured at mid waist level of the vertebral body. The following indices were obtained from above measurements, using the methods described by respective workers. The ‘ Canal body ratio’ (C/B)9: This was calculated by considering transverse diameters of vertebral body and C/B = Transverse Diameter of spinal canal/ Transverse Diameter of Vertebral Body The Spinal Index of Jones8: This is a kind of ratio of spinal canal and vertebral body dimensions and was described by Jones R.A.C. and Thomson J.L.G. (1968).50It was obtained by using the following formula.
I = CAP x CTRANS / BAP x BTRANS
Where, I – means The Spinal index of Jones, CAP – means antero-posterior diameter of spinal canal; CTRANS –means transverse diameter of spinal canal; BAP – means anteroposterior diameter of vertebral body and BTRANS – means transverse diameter of vertebral body. Mean, range and standard deviation were calculated using statistical tests. Also, the various dimensions of spinal canal and vertebral body in males and females were evaluated for statistical significance. The difference observed between means of male and female to know whether it is statistically significant, that is value of ‘P’ was calculated by applying ‘Z’ test10
RESULTS Two hundred normal plain radiographs and sixty four sets of normal lumbar vertebrae were studied The results of transverse diameter of spinal canal and vertebral body and anteroposterior diameter of spinal canal and vertebral body are shown in Tables 1 and 3. While the results of canal-body ratio and Spinal index of Jones calculated from the above mentioned measurements are shown in Tables 2 and 4. Tables 5 shows the comparison of of mean transverse diameters of spinal canal in whole population in the radiological group with that of previous studies while Table 6 shows the comparison of the anteroposterior diameters of spinal canal in whole sample size in osteological group with that of previous studies.
Table 1: The transverse diameter of spinal canal and vertebral body in both the groups of present study.
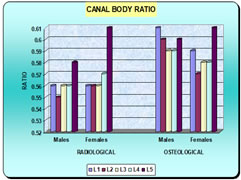
Table 2: Shows the canal- body ratio in both groups of present study (Graph 1)
Table 3: The anteroposterior diameter of spinal canal and vertebral body in both the groups of present study.
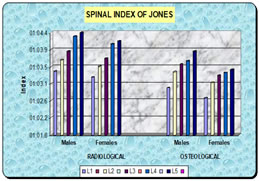
Table 4: The Spinal Index of Jones in radiological and osteological groups of the present study (Graph 2)
Graph 1 Graph 2
Table 5: Comparison of mean transverse diameters of spinal canal in whole population in the radiological group and previous studies.
Table 6: Comparison of the anteroposterior diameters of spinal canal in whole sample size in osteological group and previous studies.
DISCUSSION The mean transverse diameter of spinal canal was showing an increasing trend from L1 to L5 in both the groups. This difference in males and females is statistically highly significant. The difference in the general somatic size may be attributable to the smaller measurements in females. The mean transverse diameter of vertebral body was increasing from L1 to L5 with respect to its weight bearing functions from above downwards. The values in females were lower than males and this difference was statistically highly significant. The transverse growth of vertebral body is dependent on masculinity to some extent13. The transverse diameter of vertebral body and spinal canal is used as an index of physique expressed as canal -body ratio. Canal: body ratio showed that although the width of the vertebral body increased from L1 to L5, the width of the canal maintained a constant relationship with the size of the body at all levels. This fact is clearly of importance if differences in physique are proven to exist between different populations, e.g. males and females. Thus, it proves that the transverse diameter of spinal canal at any segmental level is proportional to the size of the vertebral body at that level8, 14. As seen in table no. 3, the canal body ratio is approximately constant at all vertebral levels i.e. 0.6. (Graph no.1) in both the groups. The mean anteroposterior diameter of the spinal canal goes on decreasing from L1 to L5. The mean values are lower in females than in males. This difference in males and females in the radiological group is statistically highly significant while in the osteological group the difference is statistically significant at L1, L4 and L5. The first lumbar vertebra lies at the level of functional transition between the relatively immobile thoracic spine and mobile lumbar spine, also it accommodates the contents at this level explaining the larger of spinal canal at L1 level. The change from lumbar to sacral type explains gradual decrease in the spinal canal15-18. The mean anteroposterior diameter of the vertebral body progressively increases from L1 to L5 The spinal index of Jones goes on increasing from L1 to L5 in both sexes in both the groups. The canal body ratio gives information about the proportion of body to corresponding spinal canal by just considering the transverse diameters. However, the spinal index gives information about the proportion of transverse diameter and anteroposterior diameters of body and corresponding spinal canal. From table nos. 1,2,3 and 4 it is seen that the mean values of transverse diameter of spinal canal, transverse diameter of vertebral body, anteroposterior diameter of vertebral body and the spinal index of Jones goes on increasing from L1 to L5. The anteroposterior diameter of spinal is decreasing from L1 to L5 in both the study group. Thus, from all the above-mentioned tables it is evident that, when a comparison of direct measurements of cadaveric lumbar vertebrae with those of radiological group is made, the anatomical values are lower than in the radiological group. This is probably due to magnification factor in the radiological group11,12. When the findings of present study were compared with previous studies (Tables 5and6) they showed regional variation mainly because of interplay of ethnic and environmental factors.
CONCLUSION In the present study, a set of normal values were obtained in radiological and an osteological group. It was found in the radiological as well as in the osteological study that, the anteroposterior and transverse diameters of spinal canal and vertebral bodies showed statistically significant differences in their mean values for males and females indicating sexual dimorphism. The spinal index of Jones also shows sexual dimorphism. When the findings obtained from radiological study were compared with those of the osteological study, it was found that the radiological findings were higher than the osteological ones. However, the canal-body ratios of these two studies remained constant. However, continuance of such studies in a defined geographic area over a period of time and its meta-analysis will be helpful in observing the changing trends in metric measurements if any. The baseline standards will have to be evaluated from time to time for their validity.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.